|
Glob Reg Health Technol Assess 2024; 11: 161-168 ISSN 2283-5733 | DOI: 10.33393/grhta.2024.3042 ORIGINAL RESEARCH ARTICLE |
Exploring the administrative burden faced by hematologists: a comprehensive study in Italy
Davide Petruzzelli1, Marco Vignetti![]() 2, Stefania Trasarti
2, Stefania Trasarti![]() 3, Paolo Sportoletti
3, Paolo Sportoletti![]() 4, Silvia Della Torre
4, Silvia Della Torre![]() 1,5, Roberto Cairoli
1,5, Roberto Cairoli![]() 6, Francesca Pia Chiara Leone7, Giuseppe Pompilio
6, Francesca Pia Chiara Leone7, Giuseppe Pompilio![]() 8, Marco Gullì9, Eva Brown Hajdukova
8, Marco Gullì9, Eva Brown Hajdukova![]() 10, Davide Integlia11
10, Davide Integlia11
ABSTRACT
Background: Administrative burdens have been identified as a major issue impacting patient care, professional practice, and the overall efficiency of healthcare systems. The aim of this study is to assess the administrative burden faced by Italian hematologists.
Methods: A cross-sectional survey that included both closed-ended quantitative questions and open-ended free text answer options was administered to 1,570 hematologists working with malignancies and members of Italian GIMEMA Foundation – Franco Mandelli ONLUS and the Italian Linfomi Foundation (FIL). The survey was conducted online from May 24 to June 30, 2023. Descriptive statistics were computed for the quantitative data to clearly summarize the responses and descriptive analysis of free text responses was carried out.
Results: Surveyed hematologists spend an average of 47.07% of their time on administrative tasks, with 63.22% (n = 110) of respondents reporting spending at least half of their time on these activities. More than half (57.47%, n = 100) reported that “Patient care” is the medical task most affected by a lack of time. Additionally, 55.17% (n = 96) reported experiencing burnout in the past 6 months, with filling out “Forms” being identified as the top contributing administrative task by 27.59% (n = 48) of respondents, followed by “Scheduling” (24.71%, n = 43) and “Managing IT system failures” (21.84%, n = 38). Nearly half of the surveyed hematologists (45.40%, n = = 79) identified patient care as the top priority requiring more time.
Conclusions: The study confirms that the administrative workload of hematologists has a significant impact on patient care, communication, and burnout risk, reducing the time available for patient care, leading to exhaustion and concern about clinical errors.
Keywords: Administrative burden, Blood cancer, Burnout, Hematology, Oncology, Survey
Received: February 8, 2024
Accepted: June 12, 2024
Published online: July 3, 2024
This article includes supplementary material
Global & Regional Health Technology Assessment - ISSN 2283-5733 - www.aboutscience.eu/grhta
© 2024 The Authors. This article is published by AboutScience and licensed under Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0).
Commercial use is not permitted and is subject to Publisher’s permissions. Full information is available at www.aboutscience.eu
Introduction
For years, physicians around the world have raised unnecessary administrative burden as an issue impacting patient care, professional practice, and the effectiveness of the overall healthcare system (1). Hematologists in Italy are no exception. Yet, despite raising the issue, seemingly larger and more critical issues have continually overshadowed concerns with increasing administrative burden. Hematologists face unique challenges and stressors due to the emotional toll of working with cancer patients and the complexity of cancer treatment (2). Evidence suggests that burnout occurs frequently in the oncology workforce (3) and commonly stems from cognitive, emotional, and administrative demands related to delivering highly complex cancer care (4). Electronic health records (EHRs) have been also shown to be a major stressor contributing to burnout and job dissatisfaction (5). Other factors associated with burnout include increased work hours, young age, poor work/life balance, mobbing (6), and increased administrative burdens (7). More importantly, unaddressed burnout is associated with adverse effects on patient care, healthcare quality and productivity, and physician health (8). Physicians who experience burnout are more likely to report medical errors (9), which can compromise the quality of care and contribute to increased healthcare costs (10). The World Health Organization (WHO) defines burnout as a clinical syndrome related to occupation, resulting from prolonged, unaddressed occupational stress. This syndrome is characterized by physical and/or emotional exhaustion, cynicism and/or depersonalization, and feelings of inefficacy or a diminished sense of professional accomplishment (11). Symptoms typically emerge when there is an imbalance between job demands and available resources, leading to physical, psychological, and emotional strain. Risk factors include occupational factors such as high patient loads, increased administrative duties, reliance on electronic medical records (EMRs), and limited social support, as well as individual factors like being female, younger in age, or not in a committed partnership (12). Burnout can also lead to physicians seeking alternative employment, quitting their medical practice, considering early retirement, and reducing their work hours, which has the potential to destabilize a practice, hospital, and healthcare system overall (13). Since the time spent on administrative work limits the hematologist’s time with patients, leading to concerns about the risk of clinical errors as highlighted by literature (8), the aim of this cross-sectional survey study was to assess the administrative burden faced by Italian hematologists and to identify if Italian hematologists are experiencing burnout and tasks contributing to burnout. The authors were unable to identify any studies to date that have been conducted in Italy quantifying the amount of time hematologists working with malignancies spend on administrative tasks or to determine whether administrative burden contributes to burnout.
Methods
Defining administrative tasks in healthcare
Administrative work is defined by task (14), task group (15), or relative value to patient care in the literature (1). However, no cohesive model of administrative work in healthcare exists to date (16). Defining administrative tasks in healthcare is challenging due to healthcare’s complex and evolving nature, varying legal and regulatory requirements, and technological advances. The perception of administrative tasks may also vary among individuals and healthcare organizations. What one facility considers an administrative task may be considered a clinical task in another. This subjectivity creates challenges when trying to standardize definitions (1).
Survey development
During the development of the survey, a conceptual model of administrative work (16) (Fig. 1) was used to clarify the concept of administrative work within the healthcare context based on prior conceptualizations of administrative work (14,15). This model divides work into three categories: patient care, patient administration, and office work. Patient care includes activities directly related to medical practice, such as diagnosis and treatment. Patient administration involves tasks with both clinical and administrative aspects, such as scheduling appointments and handling insurance issues. Office work encompasses purely administrative tasks, such as reordering supplies and troubleshooting EHR issues. This model helps to distinguish between administrative work and other types of work and highlights tasks that can be performed by nonphysician providers and staff.
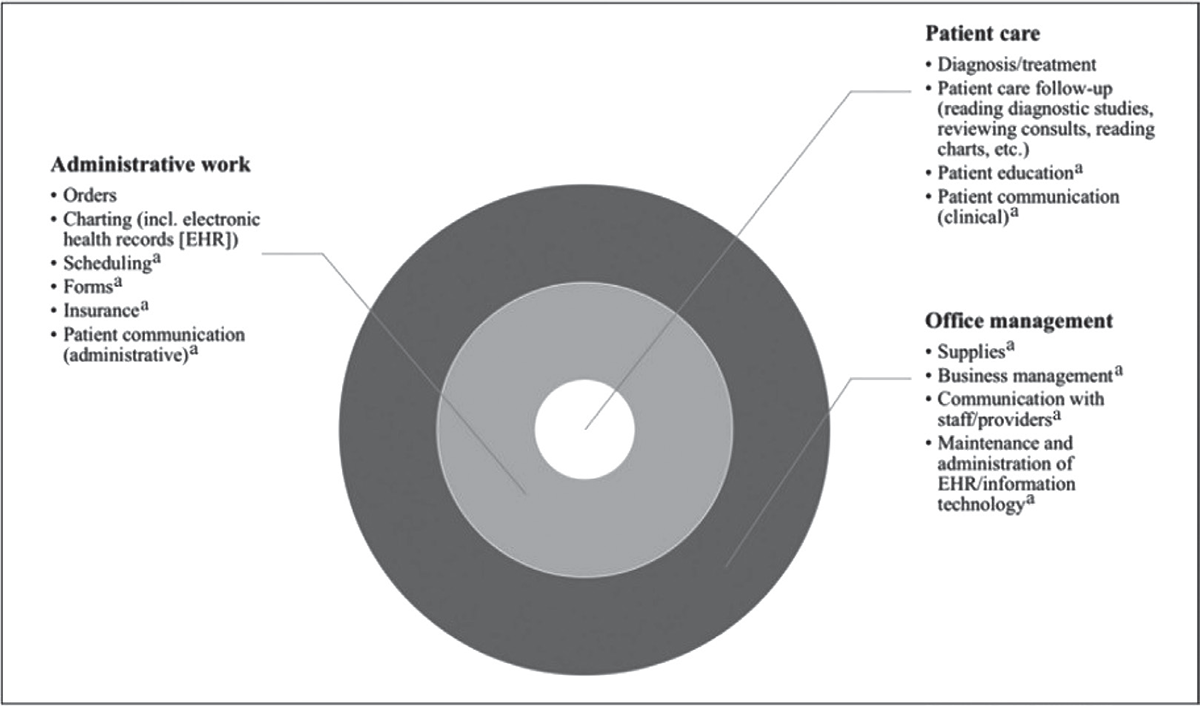
FIGURE 1 - Conceptual model of work content within healthcare.
Source: Adapted by Apaydin (16) from Chen et al (14) and Sinsky et al (15) (13).
aCan be performed by nonphysician providers or staff.
An Italian scientific committee refined the task group categories included in the conceptual model and identified missing elements, resulting in the development of two main task categories: medical tasks and administrative tasks. Expert discussions and a review of published literature indicated a strong link between high administrative burden and burnout, leading to the decision to explore this phenomenon as part of the survey. The involvement of the scientific committee from the beginning of survey development ensured a deep understanding of Italian health culture, expectations, and practices. This helped to create culturally sensitive and appropriate survey questions for the target population, increasing the likelihood of obtaining accurate and relevant responses. The research was conducted ethically with an emphasis on community engagement and participation. Involving health experts from the country of origin also helped to identify potential biases or limitations and provided valuable insights to improve the overall quality of the survey.
Study design and population
This cross-sectional survey was conducted online from May 24 to June 30, 2023. It consisted of 27 questions and was divided into five sections: About the Survey, Eligibility Screening and Informed Consent, Basic Demographic and Professional Characteristics, Administrative Tasks, and Medical Tasks. No participant identifiers were linked to the survey. Leading scientific societies and foundations in the field of hematology were invited to participate in the survey. However, participants were recruited from the Italian GIMEMA Foundation – Franco Mandelli ONLUS and the Italian Linfomi Foundation (FIL) who agreed to participate. Representatives from these foundations distributed the survey link via email to their members (1,570) who met the eligibility criteria of being hematologists working with malignancies. Reminder emails were sent by each foundation two times.
Data collection
The data collected on demographic and professional characteristics provided insight into the diversity of the hemato-oncology field and various aspects of clinical practice. The survey explored characteristics such as gender, age distribution, geographical distribution by province, years of experience in hemato-oncology, patient caseload, and the most common hematological malignancies being treated. The survey also investigated employment patterns and the use of electronic record-keeping practices within this specialized field.
Data and analysis
The survey included both closed-ended quantitative questions and open-ended free text answer options. Descriptive statistics were computed for the quantitative data to clearly summarize the responses using Microsoft Excel. Central tendency indicators, including the mean and median, were determined to identify the typical participant’s response. For the survey questions that allowed for free text responses, a descriptive analysis of the textual content was carried out. This qualitative examination involved identifying recurring themes, patterns, and sentiments expressed by the participants in their open-ended answers, following the principles of thematic analysis (17). Two authors performed the analyses independently and any disagreements were solved by discussion.
Results
A total of 182 respondents from diverse regions and healthcare settings were included in the analysis, but 8 of 182 were deleted due to exclusion criteria set out. The valid questionnaires were 174.
Demographic and professional characteristics
The respondents were predominantly female, constituting a majority of 62.07% (n = 108). Male respondents accounted for 37.93% (n = 66) of the total sample. The participants exhibited a diverse age distribution, with the largest proportion falling within the age group of 36 to 45, constituting 29.31% (n = 51) of the sample. The survey captured healthcare professionals from various provinces, with Lombardia representing the highest percentage at 21.84% (n = 38), followed by Lazio (14.94%, n = 26), Toscana (12.65%, n = 22), Veneto (9.20%, n = 16), and Emilia-Romagna (9.20%, n = 16), among others. Experience in the field varied among respondents, with the majority falling within the 5-14 years range (31.03%, n = 54). The healthcare practitioners reported diverse patient caseloads per week. The largest group treated between 45 and 64 patients (32.76%, n = 57), while other caseload brackets included 25-44 patients (18.96%, n = 33), 65-84 patients (14.37%, n = 25), 85-105 patients (17.82%, n = 31), and >105 patients (5.17%, n = 9). In terms of hematological malignancies treated, the survey respondents were predominantly engaged in treating leukemia, which accounted for 64.94% (n = 113) of cases. Other prevalent malignancies included lymphoma (59.19%, n = 103), myeloma (41.38%, n = 72), and various other hematologic malignancies (25.86%, n = 45). Most of the respondents were employed by the National Healthcare Service (NHS) as civil servants, comprising 81.61% (n = 142) of the sample. The private sector constituted 18.39% (n = 32) of the respondents. The practitioners were affiliated with diverse healthcare facilities, with the highest percentage being associated with public hospitals integrated with the university (42.53%, n = 74). The findings revealed a high adoption rate of electronic record-keeping practices among the respondents. A significant majority, 90.80% (n = 158), reported entering clinical data into registers or electronic records, while a smaller proportion, 9.20% (n = 16), indicated that they did not employ electronic record-keeping methods (Appendix, Tab. I).
Administrative burden
According to the survey results, hematologists spend a significant amount of time on administrative tasks, with an average of 47.07% of their time devoted to these activities and 52.93% to medical tasks. Furthermore, 63.22% (n = 110) of the respondents reported spending at least half of their time on administrative tasks. When asked to rank the burdensomeness of various administrative tasks (with 1 being the least burdensome and 5 being the most burdensome), filling out “Forms” was ranked as the most burdensome administrative task by 70.11% (n = 122) of respondents. The second most burdensome task was “Managing IT system failures” (60.92%, n = 106), followed by scheduling (58.62%, n = 102). “Logistics” was ranked as the least burdensome task (24.14%, n = 42), with other less burdensome tasks including “Records storage” (48.85%, n = 85) and “Placing orders” (52.87%, n = 92). On the other hand, tasks involving direct interaction with patients, such as walking them to their appointment, appear to be less burdensome (24.14%, n = 42). These results indicate that hematologists find administrative tasks such as filling out forms and managing IT system failures to be particularly burdensome. Tasks involving direct interaction with patients, such as walking them to their appointment, appear to be less burdensome, further suggesting hematologists may prefer to focus on patient care and interaction, rather than administrative tasks (Fig. 2).
When asked to select the three administrative tasks that, if delegated, would alleviate the administrative burden the most (Fig. 3), the vast majority of respondents (64.94%, n = 113) identified “Scheduling” as the top task. This was followed closely by “Filling out forms” (64.37%, n = 112) and “Managing IT system failures” (54.60%, n = 95). “Logistics” was again selected by the fewest respondents (14.37%, n = 25). These results imply that delegating scheduling tasks could significantly reduce the administrative burden on hematologists working with malignancies. Streamlining scheduling processes and making them more efficient could potentially reduce burden and improve overall efficiency. On the other hand, tasks such as logistics appear to be less of a priority for reducing the administrative burden.
More than half of the survey respondents (57.47%, n = 100) reported that “Patient care” is the medical task most affected by a lack of time (Fig. 4). The second most affected task was “Patient communication (clinical)” (48.85%, n = 85), followed by “Recording/charting medical or clinical data during or after patient visits” (42.53%, n = 74). The least affected task was “Filling out paperwork related to patient discharge from the hospital”, with 23.56% (n = 41) of respondents reporting this as an issue. These results suggest that measures should be taken to reduce the administrative burden on hematologists, as it may have a significant impact on the quality of patient care and communication, as well as on the accuracy and completeness of medical records.
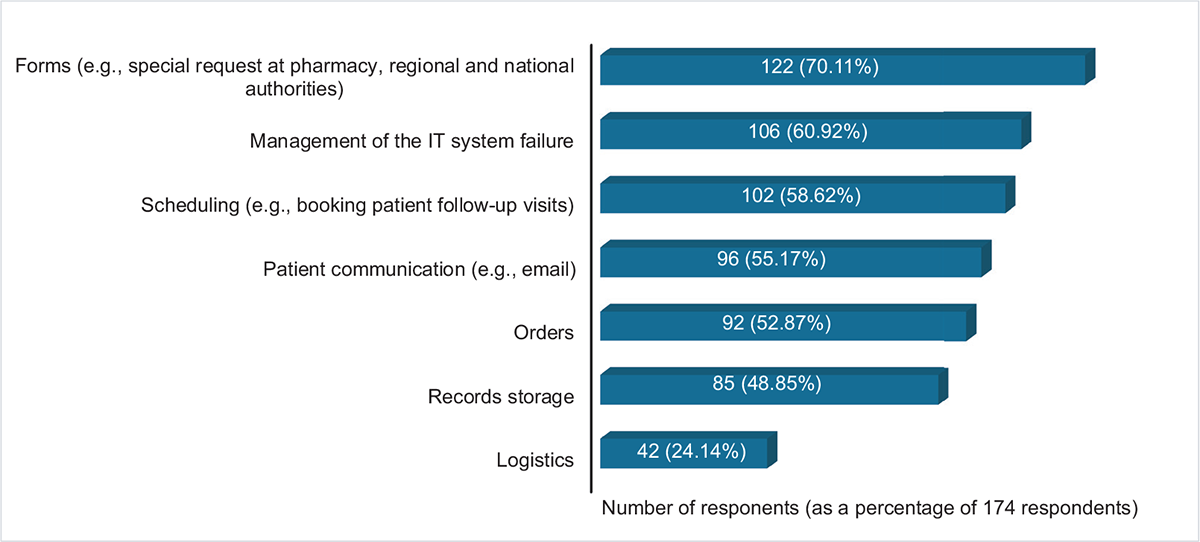
FIGURE 2 - Burdensome task ranking for administrative tasks.
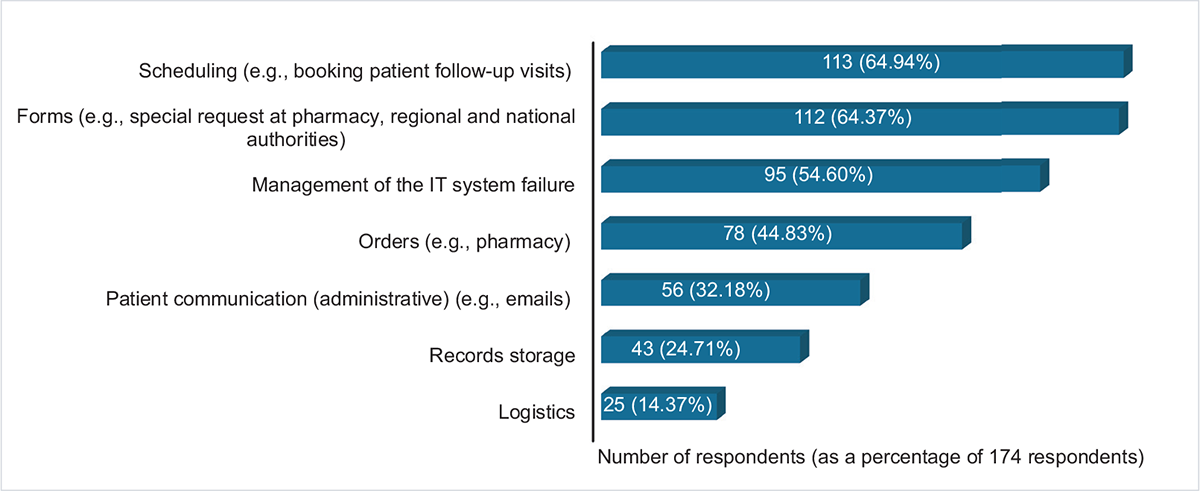
FIGURE 3 - Tasks alleviating the administrative burden the most if delegated.
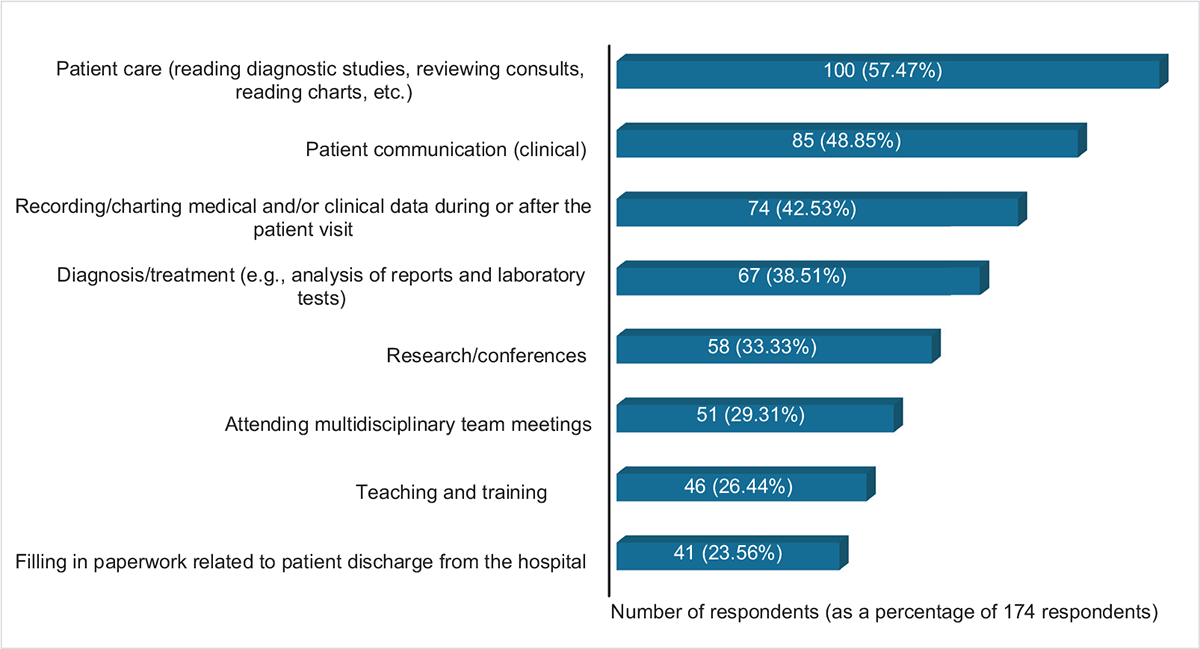
FIGURE 4 - Medical tasks most affected by lack of time (used instead for administrative activities).
Presence of burnout in the last 6 months
More than half of the survey respondents (55.17%, n = 96) reported experiencing burnout in the past 6 months. To further investigate this issue, respondents were asked to select the three tasks or activities from a list of administrative and medical tasks that had contributed the most to their sense of burnout in a multiple-choice question (Fig. 5). According to the survey results, “Filling out forms” was identified by 27.59% (n = 48) of respondents as the administrative task that contributed the most. This was followed by “Scheduling” (24.71%, n = 43) and “Managing IT system failures” (21.84%, n = 38). “Mobbing/toxic workplace” was also reported as a factor contributing toward burnout by 16.09% (n = 28) of respondents. On the other hand, “Teaching and training” was reported as contributing the least to burnout, with only 0.57% (n = 1) of respondents indicating that this task contributed to their burnout. These results indicate that healthcare organizations should consider ways to reduce the burden of paperwork and documentation on their employees in order to reduce burnout, further highlighting the need for the implementation of more efficient systems for managing paperwork, provision of additional administrative support, training for employees in completing forms, and/or reducing the amount of paperwork required. Mobbing issues also need to be addressed by implementing prevention strategies and workplace policies to improve organizational culture.
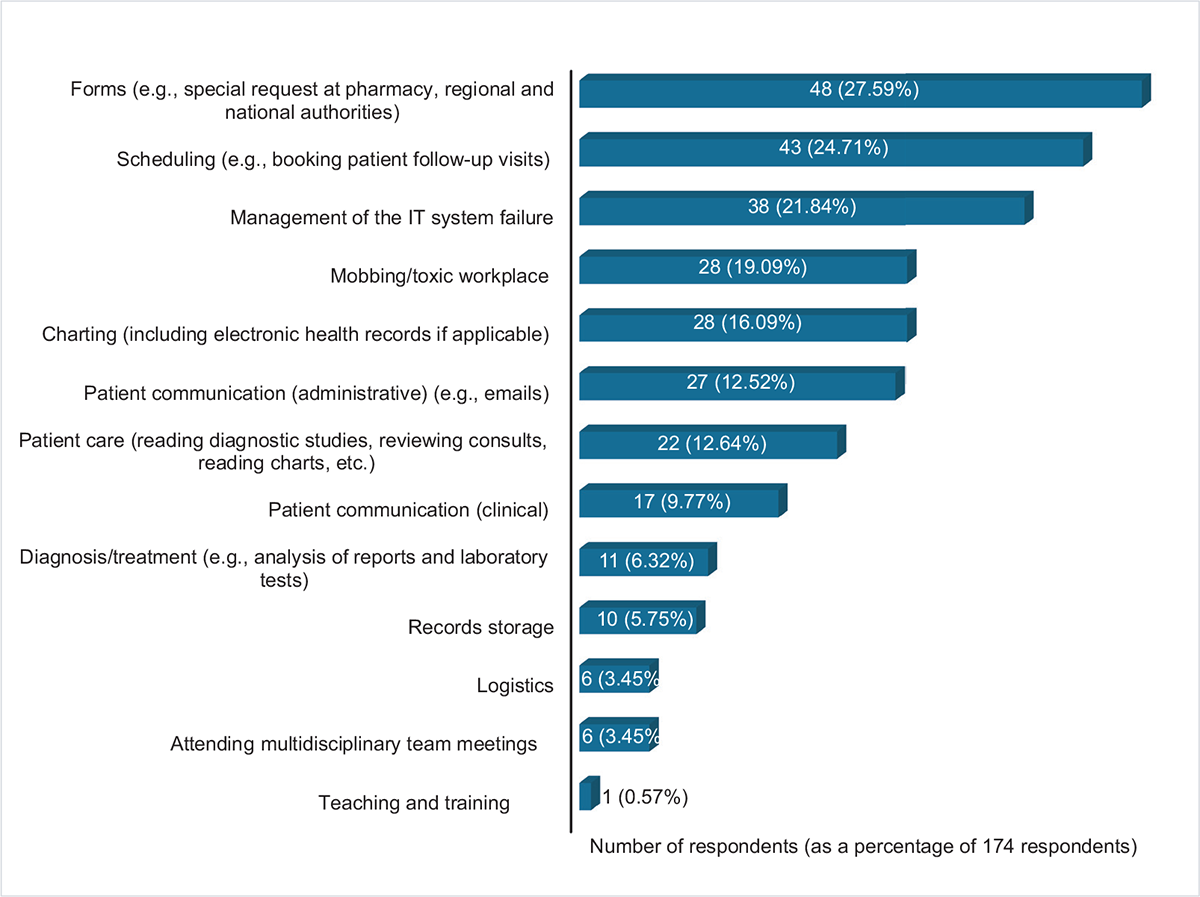
FIGURE 5 - Tasks contributing to burnout the most.
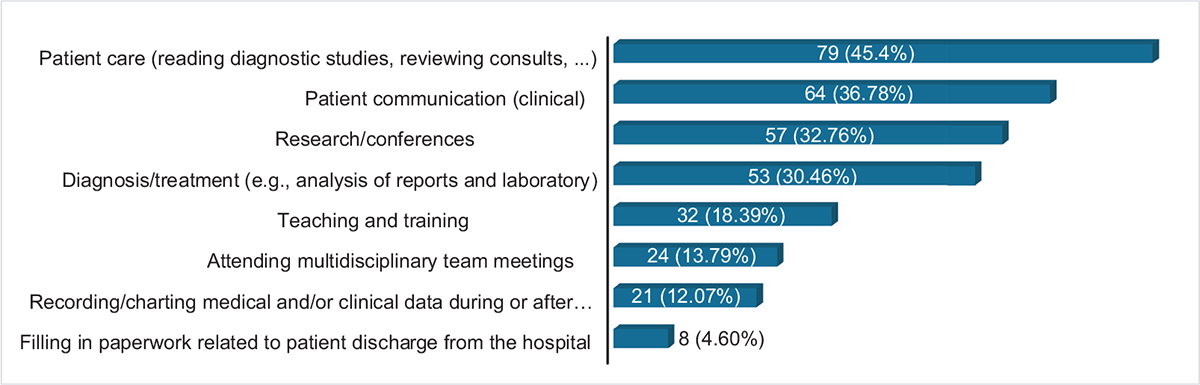
FIGURE 6 - Medical tasks that would benefit from more time.
When asked to select a medical task that would benefit from more time (Fig. 6), almost half of the survey respondents (45.40%, n = 79) identified “Patient care” as the top priority. “Patient communication” was identified by 36.78% (n = 64) of respondents, followed by “Research and conferences” (32.76%, n = 57) and “Diagnosis/treatment” (30.46%, n = 53). On the other hand, only a small percentage of respondents (4.60%, n = 8) believed that “Filling out paperwork related to patient discharge from the hospital” would benefit from more time. These results suggest that due to the high administrative burden, there is not enough time available for tasks that are essential for providing high-quality healthcare, which can lead to decreased efficiency and increased costs, as well as a potential decline in patient outcomes.
The final, “free responses” question provided respondents with an opportunity to elaborate on the impact of administrative tasks on their daily medical practice and the quality of patient care. A thematic analysis of the 36 responses revealed four key themes: professional frustration caused by performing tasks more suited to an administrative employee, balancing time for diagnosing and treating patients with avoiding clinical errors, the need for functional and efficient EHR systems, and limited time for training. These themes highlight the challenges faced by hematologists in balancing administrative tasks with their medical responsibilities and professional development and the resulting potential impact on patient care.
Discussion
The broad demographic range of the respondents provides support for the homogeneity of the responses found in the survey. The findings confirm that the significant amount of time hematologists spend on administrative tasks has a serious effect on patient care and patient communication and may be contributing to high rates of hematologists’ burnout (3). This shift in focus away from clinical tasks may have significant implications for the practice of hematology and the delivery of patient care. Mobbing is a complex type of unprofessional conduct that is also reported as a contributing factor to burnout, highlighting the need for implementing antibullying and mobbing workplace policies and guidelines as well as improving organizational culture by educating the entire staff about unprofessional and toxic behavior and its consequences (6). The complex management of time allocated for diagnosis refers to the challenges that hematologists face in balancing the time they have available for diagnosing patients with the need to avoid making clinical errors (18). This unfavorable situation often leads to increased stress and pressure, as hematologists need to carefully balance their workload to ensure that they are providing the best possible care to their patients (9). It is important for healthcare organizations to provide hematologists with the support and resources they need to effectively manage their time and avoid clinical errors.
The concept of EHRs has been consistently linked to lower job satisfaction (5,19) and physician burnout (20,21), particularly when the EHR system is complex and difficult to use (22). Management of IT system failures was reported in this study as one of the most burdensome administrative tasks contributing to burnout. This highlights the need for efficient implementation and postimplementation strategies (22) such as training, technical/educational support for users, and improving literacy and skills in technology (23). Given the direct impact of physician burnout on the delivery of high-quality healthcare, it is vital that health information technology tools are designed to minimize practice inefficiencies (20). Thematic analysis of the free text indicates hematologists’ dissatisfaction with the impact of administrative workload on their job roles, further suggesting that delegating some administrative tasks may provide a potential solution for overburdened hematologists. Arguably, the addition of staff increases costs to the healthcare system for completing the same amount of work (16). However, the cost of physician burnout due to administrative work should also be considered. Physicians experiencing burnout over time are more likely to reduce their working hours or leave the workforce (13), which can have significant societal costs (10,24). The survey findings are consistent with those reported in the National Physician Health Survey conducted by the Canadian Medical Association (CMA), which identified a significant prevalence of burnout, anxiety, depressive symptoms, and feelings of moral distress among physicians. Data from the Canadian survey underscore the association between administrative burdens and burnout. Specifically, 79% of physicians reported low levels of professional fulfillment, indicating dissatisfaction and a lack of meaning in their work. Additionally, slightly more than half of the respondents reported experiencing moral distress in their professional roles (25). Preventing burnout before it occurs, by redistributing administrative work to specialized administrative staff, may be more cost-effective than addressing its negative effects after it has already occurred. (16).
Moreover, to address and alleviate administrative burnout, it would be beneficial to implement recommendations from the American College of Physicians (ACP). These recommendations include allocating adequate financial resources to the healthcare system, critically reviewing administrative tasks that are essential for healthcare operations, and engaging scientific societies, primary care physicians, patients, and EHR providers. This collaborative effort aims to identify and implement measures that reduce unnecessary administrative burdens, ultimately enhancing the quality and efficiency of healthcare delivery (1).
Further research should be conducted to better understand potential costs such as increased healthcare costs from reduced quality of care and the cost of training new physicians to replace those leaving the workforce early. Hematologists need continuing training to keep up with the latest developments in their field. However, too much time spent on administrative tasks can crowd out other aspects of hematologists’ mission such as research and teaching as the study results indicate. A reduction in time available for professional training and teaching may impact the ability to conduct research and contribute to the advancement of the hematology field. It can also hinder preparedness for practice in increasingly complex cancer care and delivery, which can negatively influence the provision of high-quality cancer care (26).
The limitations of our study, including its potential lack of generalizability and reliance on self-reported data, are important considerations that may influence the interpretation of our results. Firstly, our survey was conducted exclusively among Italian hematologists affiliated with GIMEMA and FIL, which limits the generalizability of our findings to broader populations of hematologists or other medical specialties. The specific characteristics and experiences of hematologists associated with these organizations may not fully represent the broader hematologist community in Italy or internationally. Future research should aim to conduct more extensive and diverse sampling across various healthcare settings and regions to enhance the generalizability of findings. Secondly, the reliance on self-reported data in our survey introduces the potential for recall bias or social desirability bias. Hematologists’ perceptions of their administrative burden and its impact on burnout may be influenced by individual subjectivity or motivations. Future studies could incorporate objective measures or multiple data sources (e.g., time spent compiling administrative records) to provide a more comprehensive and nuanced understanding of the relationship between administrative burden and burnout. To tackle these challenges, future research could employ longitudinal study designs to establish temporal relationships and causal inferences between burnout onset and various outcomes, including clinical performance, medical errors, workplace mobbing, EHR usage, career decisions, job turnover, and patient satisfaction among hematologists. This approach would involve assessing changes in burnout over time, particularly following the implementation of interventions aimed at reducing administrative burden. Longitudinal studies would enable researchers to track longitudinal changes and more effectively evaluate the impact of variations in administrative workload on burnout outcomes. Additionally, employing mixed-method approaches that combine quantitative surveys with qualitative interviews or focus groups could offer richer insights into the complex interplay of administrative demands, professional satisfaction, and overall well-being among hematologists.
A more comprehensive understanding of hematologists’ burnout could be achieved through rigorous research methods, such as large-scale prospective studies that account for the complex and varied work characteristics of hematologists across different specialties. Moreover, health services research could explore the costs associated with these outcomes and the potential cost-effectiveness of interventions, or other policy reforms.
Conclusion
The findings of this study underscore the significant impact of administrative workload on hematologists’ ability to deliver optimal patient care, facilitate effective communication, and mitigate the risk of burnout. The allocation of time to administrative duties reduces the time available for patient care, precipitating fatigue and heightening concerns regarding potential clinical oversights. Moreover, the EHR has been associated with diminished job satisfaction and increased burnout rates, particularly in instances where system complexity impedes usability. Delegating administrative tasks to specialized staff emerges as a viable strategy to reduce the burden on hematologists and may be more cost-effective than addressing the negative effects of burnout after it has occurred. Although several empirical evidence on the nature and consequences of burnout among oncology professionals can be found in the literature, further research is needed to investigate the relationship between administrative burden and burnout among hematologists and the potential impact on patient care and safety.
Acknowledgments
The authors thank all clinicians for review and comments on an early version of this manuscript.
Disclosures
Conflict of interest: The authors declare no conflict of interest.
Financial support: This study was conducted with ISHEO’s own resources and the patient association “La Lampada di Aladino ETS”.
References
- 1. Erickson SM, Rockwern B, Koltov M, McLean RM; Medical Practice and Quality Committee of the American College of Physicians. Putting patients first by reducing administrative tasks in health care: a position paper of the American College of Physicians. Ann Intern Med. 2017;166(9):659-661. CrossRef PubMed
- 2. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516-529. CrossRef PubMed
- 3. Lee AI, Masselink LE, De Castro LM, et al. Burnout in US hematologists and oncologists: impact of compensation models and advanced practice provider support. Blood Adv. 2023;7(13):3058-3068. CrossRef PubMed
- 4. Weintraub AS, Sarosi A, Goldberg E, Waldman ED. A cross-sectional analysis of compassion fatigue, burnout, and compassion satisfaction in pediatric hematology-oncology physicians in the United States. J Pediatr Hematol Oncol. 2020;42(1):e50-e55. CrossRef PubMed
- 5. Bajwa NK, Singh H, De KK. Impact of EHR technology implementation on physicians’ job satisfaction. Int J Appl Manag Technol. 2019;18(1):11. CrossRef
- 6. Karsavuran S, Kaya S. The relationship between burnout and mobbing among hospital managers. Nurs Ethics. 2017;24(3):337-348. CrossRef PubMed
- 7. Murali K, Makker V, Lynch J, Banerjee S. From burnout to resilience: an update for oncologists. Am Soc Clin Oncol Educ Book. 2018;38(38):862-872. CrossRef PubMed
- 8. Hlubocky FJ, Taylor LP, Marron JM, et al. A call to action: ethics committee roundtable recommendations for addressing burnout and moral distress in oncology. JCO Oncol Pract. 2020;16(4):191-199. CrossRef PubMed
- 9. Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians: a systematic review. JAMA. 2018;320(11):1131-1150. CrossRef PubMed
- 10. Han S, Shanafelt TD, Sinsky CA, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. 2019;170(11):784-790. CrossRef PubMed
- 11. World Health Organization (WHO). Burn-out an “occupational phenomenon”: International Classification of Diseases. Online Accessed February 2024.
- 12. Hlubocky FJ, Back AL, Shanafelt TD. Addressing burnout in oncology: why cancer care clinicians are at risk, what individuals can do, and how organizations can respond. Am Soc Clin Oncol Educ Book. 2016;35(36):271-279. CrossRef PubMed
- 13. Shanafelt TD, Mungo M, Schmitgen J, et al. Longitudinal study evaluating the association between physician burnout and changes in professional work effort. Mayo Clin Proc. 2016;91(4):422-431. CrossRef PubMed
- 14. Chen MA, Hollenberg JP, Michelen W, Peterson JC, Casalino LP. Patient care outside of office visits: a primary care physician time study. J Gen Intern Med. 2011;26(1):58-63. CrossRef PubMed
- 15. Sinsky C, Colligan L, Li L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753-760. CrossRef PubMed
- 16. Apaydin E. Administrative work and job role beliefs in primary care physicians: an analysis of semi-structured interviews. Sage Open. 2020;10(1). CrossRef
- 17. Braun V, Clarke V. Is thematic analysis used well in health psychology? A critical review of published research, with recommendations for quality practice and reporting. Health Psychol Rev. 2023;17(4):695-718. CrossRef PubMed
- 18. Menon NK, Shanafelt TD, Sinsky CA, et al. Association of physician burnout with suicidal ideation and medical errors. JAMA Netw Open. 2020;3(12):e2028780-e2028780. CrossRef PubMed
- 19. Nguyen OT, Jenkins NJ, Khanna N, et al. A systematic review of contributing factors of and solutions to electronic health record-related impacts on physician well-being. J Am Med Inform Assoc. 2021;28(5):974-984. CrossRef PubMed
- 20. Downing NL, Bates DW, Longhurst CA. Physician burnout in the electronic health record era: are we ignoring the real cause? Ann Intern Med. 2018;169(1):50-51. CrossRef PubMed
- 21. Micek MA, Arndt B, Tuan WJ, et al. Physician burnout and timing of electronic health record use. ACI Open. 2020;4(1):e1-e8. CrossRef PubMed
- 22. Shanafelt TD, Dyrbye LN, Sinsky C, et al. Relationship between clerical burden and characteristics of the electronic environment with physician burnout and professional satisfaction. Mayo Clin Proc. 2016;91(7):836-848. CrossRef PubMed
- 23. Tsai CH, Eghdam A, Davoody N, Wright G, Flowerday S, Koch S. Effects of electronic health record implementation and barriers to adoption and use: a scoping review and qualitative analysis of the content. Life (Basel). 2020;10(12):327. CrossRef PubMed
- 24. Dewa CS, Jacobs P, Thanh NX, Loong D. An estimate of the cost of burnout on early retirement and reduction in clinical hours of practicing physicians in Canada. BMC Health Serv Res. 2014 Jun 13;14:254. CrossRef PubMed
- 25. Canadian Medical Association 2021 National Physician Health Survey. Online Accessed February 2024.
- 26. Roberts DA, Faig J, Bodio-Downey K, et al. Training hematologists/oncologists for the academic-community hybrid: creating a fellowship framework for the future. JCO Oncol Pract. 2023;19(6):e927-e934. CrossRef PubMed