|
Glob Reg Health Technol Assess 2024; 11: 82-93 ISSN 2283-5733 | DOI: 10.33393/grhta.2024.2697 ORIGINAL RESEARCH ARTICLE |
The socioeconomic burden of adult attention-deficit/hyperactivity disorder in Spain
María Merino![]() 1, Paulina Maravilla-Herrera
1, Paulina Maravilla-Herrera![]() 1, Teresa Martín Lorenzo
1, Teresa Martín Lorenzo![]() 1, Juan Antonio Arance2, Julio Bobes
1, Juan Antonio Arance2, Julio Bobes![]() 3-7, Montse Corrales8, Fátima Guzmán9, María Morales10, Carlos Mur11
3-7, Montse Corrales8, Fátima Guzmán9, María Morales10, Carlos Mur11
ABSTRACT
Introduction: The symptoms of attention-deficit/hyperactivity disorder (ADHD) in adults highly interfere with function in multiple dimensions, increasing the economic burden associated with ADHD. The aim of this study was to explore the impact of ADHD in Spanish adults and estimate the associated economic burden within the healthcare, social, economic, and legal domains.
Methods: An economic model was developed from a social perspective using a bottom-up approach, based on the scientific literature and a multidisciplinary expert group.
Results: The cost incurred per diagnosed adult patient with ADHD included an annual cost of €15,652 and a one-time cost of €7,893 (3,035 M€ and 1,531 M€ for Spain, respectively). Regarding the annual cost, 50% was attributed to costs within the economic domain, of which 53% were work-absenteeism-related. Moreover, 28% was attributed to costs within the social domain, of which 74% were substance-abuse-related. Regarding the one-time cost, 52% was attributed to costs within the healthcare domain, of which approximately 50% were hospitalization-related costs. Moreover, 42% was attributed to costs within the legal domain, of which 62% were imprisonment-related costs.
Conclusions: This is the first report on the socioeconomic burden of ADHD in Spanish adults, shedding light on the large burden that adult ADHD poses on the healthcare system and society at large, as symptoms have been shown to impact almost every aspect of life. This is particularly important for undiagnosed/untreated patients with ADHD in Spain, as appropriate treatments have shown positive results in these areas and may reduce its associated socioeconomic burden.
Keywords: adult ADHD, burden of disease, healthcare system, social perspective, substance abuse, work productivity loss
Received: October 25, 2023
Accepted: March 15, 2024
Published online: April 5, 2024
Global & Regional Health Technology Assessment - ISSN 2283-5733 - www.aboutscience.eu/grhta
© 2024 The Authors. This article is published by AboutScience and licensed under Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0).
Commercial use is not permitted and is subject to Publisher’s permissions. Full information is available at www.aboutscience.eu
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by a persistent pattern of inattention, hyperactivity, and/or impulsivity that interferes with functioning or development, with symptoms present before the age of 12, in two or more settings, and not exclusively related to other mental disorders (1). The main characteristics of ADHD encompass symptoms of inattention (e.g., forgetfulness, distractibility, doubtfulness, etc.), hyperactivity (e.g., restlessness, difficulty relaxing, talking too much and too loud, etc.), and impulsivity (e.g., acting without thinking, interrupting others, impatience, etc.), which pose a substantial burden on patients and society at large (2).
Typically diagnosed in early childhood, ADHD is among the most common group of mental disorders in children and adolescents with a worldwide pooled prevalence of 3.4% (3). However, considered a lifespan disorder (2), ADHD may persist into adulthood (57.0%-78.2%) as patients continue to meet the criteria for ADHD as adults (4). Accordingly, the worldwide pooled prevalence of adult ADHD has been estimated at 2.8% of the total population (4).
The latest update on ADHD diagnostic criteria specified the need for clear evidence that symptoms interfere with or reduce the quality of social, academic, or occupational functioning (1,2). While children with ADHD present social and academic difficulties, impairments in adults with ADHD extend beyond these areas (1). Specifically, adults with ADHD present social and interpersonal difficulties such as unstable relationships and marital problems leading to separation or divorce; work-related problems such as unemployment and underachievement; and antisocial and criminal behavior leading to arrests, convictions, and/or imprisonment, among others (2,5). Accordingly, a recent systematic review showed that adults incur most of the economic burden associated with ADHD (89.5%) compared to that incurred by children and adolescents (10.5%) (6). In this regard, most ADHD economic burden studies have typically examined only direct costs (medical and nonmedical costs), followed by indirect costs (indirect medical costs, absenteeism, presentism), and a paucity of studies have further captured educational or justice system associated costs, hence underestimating the real economic burden (7). However, particularly for adults, the multidimensional impact of ADHD on function prompts an analysis encompassing a greater number of domains (e.g., healthcare, social, academic, occupational, etc.) to provide a comprehensive description of the economic burden of adult ADHD (2,7).
Impaired functioning associated with ADHD may be prevented or mitigated by an appropriate multimodal treatment (8). Specifically, pharmacological treatment of ADHD (i.e., methylphenidate, lisdexamfetamine, and atomoxetine) has been reported to be both effective and well-tolerated, and has shown a positive impact on important aspects of daily functioning (8). Unfortunately, adult ADHD is often underdiagnosed or misdiagnosed due to the overlap of symptoms with other psychiatric disorders and hence undertreated (9). Moreover, the difficult transition from pediatric to adult healthcare services may compromise treatment continuity (8). These patients continue to show greater healthcare utilization and economic burden compared to those without ADHD (10). Consequently, untreated adult patients with ADHD highly contribute to the overall burden associated with ADHD.
While the socioeconomic burden of children and adolescents with ADHD in Spain has been previously studied (11), we are unaware of any previous study on the socioeconomic burden of adult ADHD in Spain (7). Given that childhood-onset ADHD may persist into adulthood (4) and enhance the socioeconomic burden of ADHD (7), this should be studied in detail across relevant domains. Therefore, the aims of the present study were to identify the most relevant impacts of ADHD in the adult population of Spain and to estimate their associated burden within the healthcare, social, economic, and legal domains.
Methods
The burden of adult ADHD in Spain was estimated through an economic model developed from a social perspective using a bottom-up approach and divided into four domains (Fig. 1).
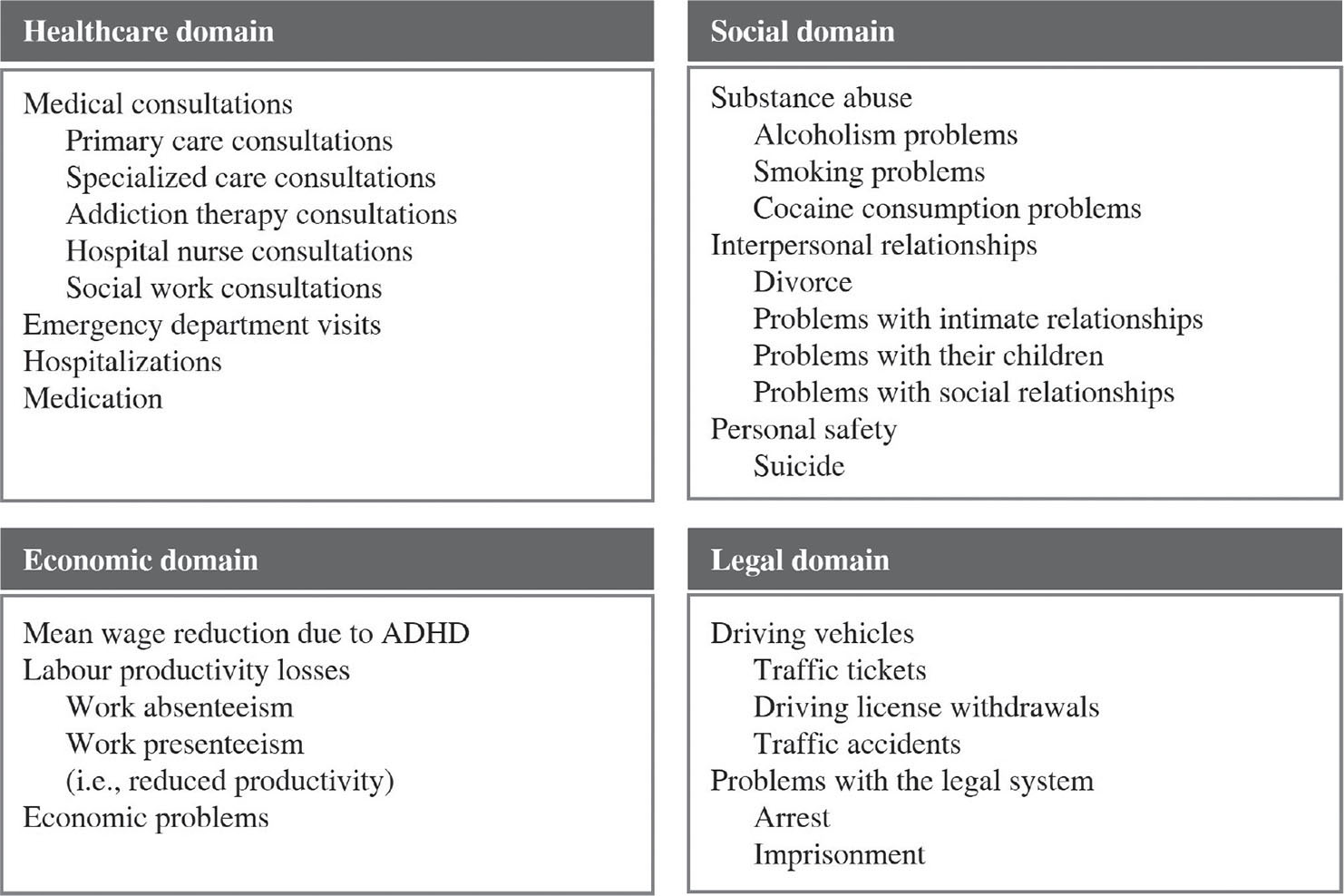
FIGURE 1- Study domains and associated variables. ADHD = attention-deficit/hyperactivity disorder.
Data sources
Relevant data regarding the prevalence of adult ADHD in Spain and its impact on the healthcare, social, economic, and legal domains were obtained from the scientific literature using the PubMed search engine and selected based on their representation of Spain or any of its regions, or, otherwise, on study methodology. Thereafter, an Advisory Board of a multidisciplinary group of experts on ADHD, including a hospital psychiatric department chief, a prison health service physician, a hospital psychiatric department psychologist, a mental health service social worker, the director of the ADHD association of patients, and a former hospital manager and psychiatrist, was convened to agree on which of the presented data points were to be included in the socioeconomic model. Whenever experts considered that a data point was not representative of the Spanish adult population with ADHD and/or no alternative data point was available in the scientific literature, especially regarding healthcare resource consumption, assumptions were made.
Population
Estimates of the burden of diagnosed and undiagnosed ADHD were based on prevalence data. Accordingly, to estimate the burden of diagnosed adult ADHD in Spain, a 0.5% prevalence was used (12). Moreover, to estimate the burden of undiagnosed adult ADHD in Spain, the difference between the estimated prevalence of adult ADHD in Spain (3.3%) (4) and the prevalence of diagnosed adult ADHD in Spain (0.5%) was used, yielding a prevalence of 2.8%. Applied to the adult population of Spain (≥18 years) on July 1, 2019 (13), it was estimated that, at the time, there were 1,279,861 adults with ADHD in Spain, of which 193,918 were diagnosed (15%) and 1,085,943 were undiagnosed (85%).
Costs
The economic model included two types of costs, one-time and recurrent annual costs, given the characteristics of the first, which are timely and lack an annual frequency. Costs are of tangible and/or intangible nature, the latter of which were estimated from financial proxies (e.g., willingness to pay for an effective alcoholism therapy). Overall, healthcare costs were estimated by multiplying the number of annual resources consumed by their unit costs, while the remaining costs were estimated by further applying prevalence reference data (e.g., multiplying the prevalence of addictions in patients with ADHD by the number of annual addiction therapy consultations and their unit cost). Estimates of the healthcare burden associated with ADHD medication were based on the cost of treating an average patient with each one of the active agents used to treat ADHD and their market share (14), considering that between 10.0% and 27.3% of adult patients with ADHD are undergoing treatment (based on estimates by the Advisory Committee and Takeda, respectively). For each active agent, the presentations with the maximum daily dose as detailed in their summary of product characteristics were selected (15-17), and among them, the ones with the lowest cost per mg (retail price + taxes) (18). Moreover, costs associated with labor productivity were estimated using the human-capital method, by which work time lost as a result of illness is valued at the market wage. A detailed description of the variables and unit costs included in the socioeconomic model has been provided in Tables 1 and 2.
Unit costs were obtained from the median rates for health services published in the official bulletins of the Spanish Autonomous Communities, official statistics (published by the Spanish National Institute of Statistics and the Spanish Ministry of Health, Consumer Affairs, and Social Welfare), the scientific literature, and market prices. Prices were updated to 2019 Euro according to the corresponding general or medical Consumer Price Index (19), except for medication costs, which were obtained on September 10, 2020, from the medication database of the General Council of Official Associations of Pharmacists.
Results are presented as mean costs per adult patient with ADHD and total costs of ADHD within domains, broken down into one-time costs and recurrent annual costs. Moreover, to estimate the burden of ADHD on the healthcare system, the analysis was broken down into three distinct time periods to account for differences in resource consumption: diagnosis, post-diagnosis follow-up (first year), and post-diagnosis long-term follow-up (following years). While the diagnosis time period and the first year after diagnosis incurred one-time costs, the following years were associated with recurrent annual costs. Results are also presented as total costs of adult ADHD in Spain, which were obtained by multiplying the mean cost per patient by the prevalence of diagnosed and/or undiagnosed ADHD according to the bottom-up method (4,13). Given the lack of studies on the consumption of healthcare resources by undiagnosed adults with ADHD, the one-time and annual total cost of undiagnosed ADHD was obtained by excluding healthcare costs from the one-time and annual cost per adult patient diagnosed with ADHD and applying such costs to the estimated number of undiagnosed adults with ADHD.
Sensitivity analysis
A sensitivity analysis on assumption-based data points was carried out to account for worst and best-case scenarios, relative to a reference scenario (Tabs 1 and 2).
Results
Overall, the total cost incurred per adult patient diagnosed with ADHD included an annual cost of €15,652 and a one-time cost of €7,893. On the one hand, the annual cost was mainly attributed to costs within the economic domain (49.80%), followed by the social domain (28.35%), the healthcare domain (21.70%), and the legal domain (0.15%). On the other hand, the one-time cost was mainly attributed to costs within the healthcare domain, which accounted for those associated with diagnosis and the first year of post-diagnosis follow-up (52.08%), followed by the legal domain (42.45%), and the social domain (5.46%). Applied to the number of adult patients diagnosed with ADHD in Spain, the estimated costs would yield a total annual cost of €3,035 million and a one-time cost of €1,531 million (Tab. 3).
| Variable | Best scenario | Reference scenario | Worst scenario | Resource/financial proxy | Unit cost (€, 2019 Euro) | Cost typology | |
|---|---|---|---|---|---|---|---|
| Healthcare domain | Diagnosis | ||||||
| Medical consultations | |||||||
| Number of specialized care consultations (27) | 3.8 | 3.8 | 3.8 | First specialized care consultation‡ | 151.8 | One-time | |
| Post-diagnosis (first year) | |||||||
| Medical consultations | |||||||
| Number of annual primary care consultations† | 6.0 | 7.0 | 8.0 | Follow-up consultation with a primary care physician‡ | 50.1 | One-time | |
| Number of annual psychiatric consultations† | 4.0 | 5.0 | 6.0 | Follow-up specialized care consultation‡ | 88.3 | One-time | |
| Number of annual addiction therapy consultations†§ | 12.0 | 12.0 | 12.0 | Follow-up specialized care consultation‡ | 88.3 | One-time | |
| Number of annual hospital nurse consultations†¶ | 1.0 | 1.0 | 1.0 | Hospital nurse consultation‡ | 42.0 | One-time | |
| Number of annual social work consultations† | 1.0 | 1.0 | 1.0 | Social work consultation‡ | 36.3 | One-time | |
| Medication | |||||||
| Maximum daily adult methylphenidate dose (mg) (16) | 80.0 | 80.0 | 80.0 | Cost per mg of methylphenidate (retail price + taxes) (16,18) | 0.03403 | One-time | |
| Maximum daily adult atomoxetine dose (mg) (17) | 100.0 | 100.0 | 100.0 | Cost per mg of atomoxetine (retail price + taxes) (17,18) | 0.02603 | One-time | |
| Maximum daily adult lisdexamfetamine dose (mg) (15) | 70.0 | 70.0 | 70.0 | Cost per mg of lisdexamfetamine (retail price + taxes) (15,18) | 0.05553 | One-time | |
| ED visits and hospitalizations | |||||||
| Patients visiting the ED in the last 6 months# (28) | 30.2% | 30.2% | 30.2% | Hospital ED visit‡ | 182.2 | One-time | |
| Patients hospitalized in the last 6 months# (28) | 26.0% | 26.0% | 26.0% | Hospitalization (29) | 3,509.7 | One-time |
All variables refer specifically to patients with ADHD.
ADHD = attention-deficit/hyperactivity disorder; ED = emergency department.
†Advisory board.
‡Median rates for health services published in the official bulletins of the Spanish Autonomous Communities.
§Applies to the percentage of ADHD patients with addiction.
¶Applies to the percentage of patients undergoing treatment with stimulant medication who present with high blood pressure.
#Two annual consumptions were assumed for this resource.
| Variable | Best scenario | Reference scenario | Worst scenario | Resource/financial proxy | Unit cost(€, 2019 Euro) | Cost typology | |
|---|---|---|---|---|---|---|---|
| Healthcare domain | Medical consultations | ||||||
| Number of annual primary care consultations† | 4.0 | 5.0 | 6.0 | Follow-up consultation with a primary care physician‡ | 50.1 | Recurrent | |
| Number of annual psychiatric consultations† | 4.0 | 5.0 | 6.0 | Follow-up specialized care consultation‡ | 88.3 | Recurrent | |
| Number of annual addiction therapy consultations†§ | 12.0 | 12.0 | 12.0 | Follow-up specialized care consultation‡ | 88.3 | Recurrent | |
| Medication | |||||||
| Maximum daily adult methylphenidate dose (mg) (16) | 80.0 | 80.0 | 80.0 | Cost per mg of methylphenidate (retail price + taxes) (16,18) | 0.03403 | Recurrent | |
| Maximum daily adult atomoxetine dose (mg) (17) | 100.0 | 100.0 | 100.0 | Cost per mg of atomoxetine (retail price + taxes) (17,18) | 0.02603 | Recurrent | |
| Maximum daily adult lisdexamfetamine dose (mg) (15) | 70.0 | 70.0 | 70.0 | Cost per mg of lisdexamfetamine (retail price + taxes) (15,18) | 0.05553 | Recurrent | |
| ED visits and hospitalizations | |||||||
| Patients visiting the ED in the last 6 months¶ (28) | 30.2% | 30.2% | 30.2% | Hospital ED visit‡ | 182.2 | Recurrent | |
| Patients hospitalized in the last 6 months¶ (28) | 26.0% | 26.0% | 26.0% | Hospitalization (29) | 3,509.7 | Recurrent | |
| Social domain | Substance abuse | ||||||
| Patients who were ever alcoholics (28) | 19.6% | 19.6% | 19.6% | Annual WTP for a 100% effective alcoholism treatment# | 4,800.0 | Recurrent | |
| →Patients’ annual WTP# (30) | 1,200.0 | ||||||
| → Caregivers’ annual WTP# (30) | 3,600.0 | ||||||
| Patients who smoke (28) | 48.3% | 48.3% | 48.3% | Annual cost for treating a patient with COPD# (31) | 4,245.2 | Recurrent | |
| Patients who consume cocaine (32) | 20.8% | 20.8% | 20.8% | Annual cost for addiction rehabilitation treatment# (33) | 1,456.2 | Recurrent | |
| Interpersonal relationships | |||||||
| Patients who are divorced (32) | 8.9% | 8.9% | 8.9% | Cost of a contentious divorce# | 4,840.0 | One-time | |
| → Cost of a contentious divorce for the patient# (34) | 2,420.0 | ||||||
| → Cost of a contentious divorce for the partner# (34) | 2,420.0 | ||||||
| Patients with intimate relationship problems (35) | 59.0% | 59.0% | 59.0% | Cost of 14 psychotherapy sessions (couple’s therapy)‡# (36) | 1,236.2 | Recurrent | |
| Patients who have problems with their children (35) | 15.0% | 15.0% | 15.0% | Cost of six psychotherapy sessions (family therapy)‡# | 529.8 | Recurrent | |
| Patients with social relationship problems (28) | 63.2% | 63.2% | 63.2% | Cost of six psychotherapy sessions (individual therapy)‡# | 529.8 | Recurrent | |
| Personal safety | |||||||
| Odds ratio of suicide vs. non-ADHD (37) | 2.5 | 5.9 | 14.3 | Social and work-related cost of suicide per person (38) | 618.1 | One-time | |
| Economic domain | Mean wage reduction compared with non-ADH†† (39) | 20.0% | 20.0% | 20.0% | Annual earnings per employee in Spain (40) | 24,197.6 | Recurrent |
| Labor productivity losses | |||||||
| Absenteeism as annual days on work leave†† (41) | 33.6 | 33.6 | 33.6 | Earnings per day of work (42) | 123.8 | Recurrent | |
| Percentage of patients with work presenteeism†† (28) | 45.8% | 45.8% | 45.8% | Annual cost of presenteeism‡‡ (43) | 1,950.5 | Recurrent | |
| → Daily effective work minutes lost (43) | 15.0 | 30.0 | 45.0 | ||||
| Economic problems | |||||||
| Patients with economic problems (35) | 49.0% | 49.0% | 49.0% | Interest cost linked to personal loans (9% interest rate)# (44) | 545.9 | Recurrent | |
| Legal domain | Driving vehicles | ||||||
| Patients with >1 traffic ticket in the last 12 months (27) | 17.6% | 17.6% | 17.6% | Cost of a speeding ticket (45) | 132.0 | Recurrent | |
| Mean number of driving license withdrawals (46) | 1.1 | 1.1 | 1.1 | Cost of a driving license withdrawal | 998.5 | One-time | |
| → Very serious speeding ticket + 6-point withdrawal (47) | 600.0 | ||||||
| → Driving license recovery course (48) | 398.5 | ||||||
| Patients involved in traffic accidents while driving (27) | 18.5% | 18.5% | 18.5% | Annual insurance cost increase for traffic accidents# (49,50) | 110.2 | One-time | |
| Problems with the legal system | |||||||
| Patients who have ever been arrested | 37.0% (51) | 42.0%* | 47.0% (52) | Cost of legal counsel for criminal detainee assistance# (53) | 350.0 | One-time | |
| Patients who have ever been imprisoned | 3.5% (41) | 9.2%* | 15.0% (52) | Cost per day per inmate (54) | 61.8 | One-time |
All variables refer specifically to patients with ADHD.
ADHD = attention-deficit/hyperactivity disorder; COPD = chronic obstructive pulmonary disease; ED = emergency department; WTP = willingness to pay.
*Average of best- and worst-case scenarios.
†Advisory board.
‡Median rates for health services published in the official bulletins of the Spanish Autonomous Communities.
§Applies to the percentage of ADHD patients with addiction.
¶Two annual consumptions were assumed for this resource.
#Financial proxy.
††Applies to the percentage of patients with ADHD who are currently employed.
‡‡Cost subject to best- and worst-case scenario of daily effective work minutes lost in patients with ADHD.
| Domains/type of cost | Cost per patient(€, 2019 Euro) | Total cost†(M€, 2019 Euro) | Relative cost (%) |
|---|---|---|---|
| Healthcare burden | |||
| Recurrent annual cost | 3,395.83 | 658.51 | 21.70 |
| One-time cost‡ | 4,110.88 | 797.17 | 52.08 |
| Social burden | |||
| Recurrent annual cost | 4,437.80 | 860.57 | 28.35 |
| One-time cost | 430.99 | 83.58 | 5.46 |
| Economic burden | |||
| Recurrent annual cost | 7,794.79 | 1,511.55 | 49.80 |
| One-time cost | 0.00 | 0.00 | 0.00 |
| Legal burden | |||
| Recurrent annual cost | 23.23 | 4.51 | 0.15 |
| One-time cost | 3,350.84 | 649.79 | 42.45 |
| Total cost | |||
| Recurrent annual cost | 15,651.66 | 3,035.14 | 100 |
| One-time cost | 7,892.71 | 1,530.54 | 100 |
ADHD = attention-deficit/hyperactivity disorder; M€ = million Euros.
†Cost per patient applied to the prevalence of diagnosed adult patients with ADHD.
‡Includes costs associated with the diagnosis and the first-year post-diagnosis.
Moreover, undiagnosed patients with ADHD were estimated to incur at least a total annual cost of €13,309 million and a one-time cost of €4,107 million.
Healthcare burden
The estimated cost per adult patient with ADHD to establish a diagnosis amounted to €577, increased up to €3,534 in the first year following diagnosis, and slightly decreased to €3,396 per year during the following years. Costs associated with hospitalizations accounted for approximately 50% of the burden on the healthcare system for both the first and the following post-diagnosis years (Fig. 2A).
Social burden
The estimated cost per adult patient with ADHD within the social domain amounted to an annual cost of €4,438 and a one-time cost of €431. Costs associated with substance abuse accounted for 74.23% of the annual social burden, specifically those associated with smoking (46.20%) and alcoholism (21.20%). In addition, problems with intimate relationships accounted for 16.44% of the social burden. Moreover, the cost of a divorce at any given time in the patients’ life further contributed to the overall social burden (Fig. 2B).
Economic burden
The estimated cost per adult patient with ADHD within the economic domain amounted to an annual cost of €7,795, of which 53.35% were costs associated with work absenteeism, followed by wage reductions with respect to those without ADHD (31.76%) and work presenteeism (11.46%). One-time costs were not identified within this domain (Fig. 2C).
Legal burden
The estimated cost per adult patient with ADHD within the legal domain amounted to an annual cost of €23 associated with traffic tickets. Most importantly, one-time costs amounted to €3,351, of which 62.23% were associated with imprisonment and 32.78% with driving license withdrawals at any given time in the patients’ life (Fig. 2D).
Sensitivity analysis
Overall, the results of the sensitivity analysis showed that recurrent annual costs associated with diagnosed adults with ADHD could vary up to 6%, while one-time costs could vary up to 21% with respect to the reference scenario. More specifically, one-time costs associated with the legal domain could vary up to 39% with respect to the reference scenario (Tab. 4). This large variation within the legal system was primarily associated with variations in the percentage of patients with ADHD who have ever been imprisoned (3.5% to 15%). Moreover, the mean cost per day of imprisonment depends on the number of years that the patient spends in prison, which could further increase variability.
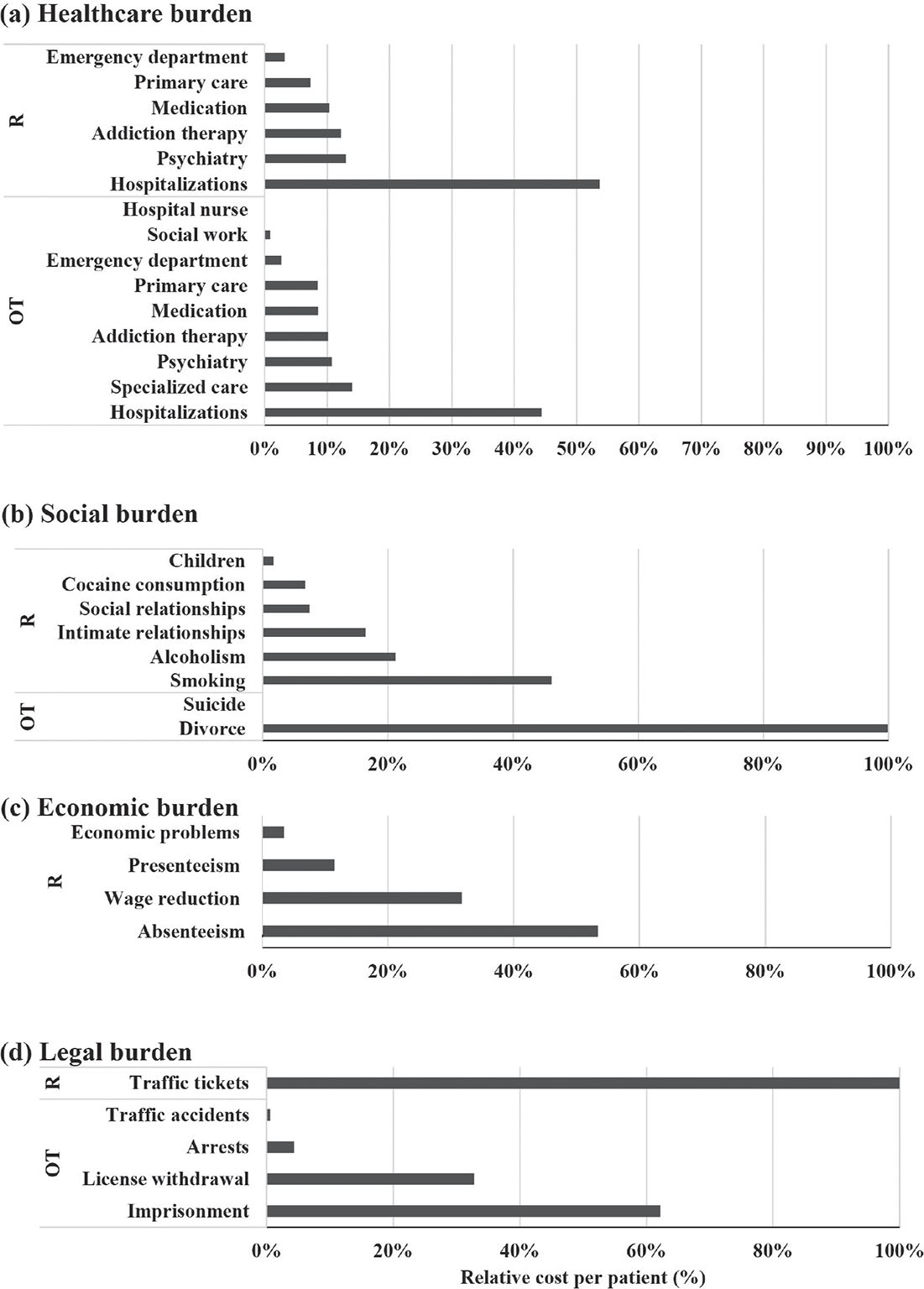
FIGURE 2 - Relative costs per patient (%) with respect to total one-time (OT) or recurrent (R) total cost within the healthcare (A), social (B), economic (C), and legal (D) domains.
This is the first report on the socioeconomic burden of adult ADHD in Spain (7). The results highlight a large socioeconomic impact, which was estimated to incur an annual cost of €15,652 and a one-time cost of €7,893 per adult patient diagnosed with ADHD (€3,035 million and €1,531 million for Spain, respectively). Given the large rates of adult ADHD underdiagnosis, estimated at 2.8% (4), the socioeconomic impact is expected to be much higher (at least €13,309 million and €4,107 million, respectively). These results are not easily comparable to previous studies on the economic burden of ADHD. A recent systematic review on the global economic burden of ADHD reported a large variability across countries possibly associated with differences in healthcare systems, resource utilization, cost components, populations, and data sources (7). Therefore, any comparisons with previous studies should be interpreted with caution.
| Domains/type of cost | Cost per patient(€, 2019 Euro) | Total cost†(M€, 2019 Euro) | |||
|---|---|---|---|---|---|
| Best-case Scenario | Worst-case Scenario | Best-case Scenario | Worst-case Scenario | ||
| Healthcare burden | |||||
| Recurrent annual cost | 3,093.32 | 3,698.35 | 599.85 | 717.18 | |
| One-time cost‡ | 3,806.94 | 4,415.68 | 738.24 | 856.28 | |
| Social burden | |||||
| Recurrent annual cost | 4,437.80 | 4,437.80 | 860.57 | 860.57 | |
| One-time cost | 430.81 | 431.62 | 83.54 | 83.70 | |
| Economic burden | |||||
| Recurrent annual cost | 7,147.29 | 8,442.29 | 1,385.99 | 1,637.12 | |
| One-time cost | 0.00 | 0.00 | 0.00 | 0.00 | |
| Legal burden | |||||
| Recurrent annual cost | 23.23 | 23.23 | 4.51 | 4.51 | |
| One-time cost | 2,033.50 | 4,668.18 | 394.33 | 905.25 | |
| Total cost | |||||
| Recurrent annual cost | 14,701.64 | 16,601.68 | 2,850.92 | 3,219.37 | |
| One-time cost | 6,271.25 | 9,515.48 | 1,216.11 | 1,845.23 | |
ADHD = attention-deficit/hyperactivity disorder; M€ = million Euros.
†Cost per patient applied to the prevalence of diagnosed adult patients with ADHD.
‡Includes costs associated with the diagnosis and the first-year post-diagnosis.
Overall, the estimated total annual cost per adult patient diagnosed with ADHD in Spain was above previous reports ranging between $US 831 (€536) to $US 20,538 (€13,247) per person (7,20). Moreover, the present study included one-time costs that increased the overall burden of adult ADHD in Spain, providing a more holistic estimate of costs. However, while previous studies on the economic burden of ADHD have typically focused on only one aspect of cost (e.g., healthcare costs) (7), the present study examined the burden of adult ADHD from a multidimensional perspective, estimating costs incurred within the healthcare, social, economic, and legal domains. Particularly important for adults with ADHD, this multidimensional analysis provides a more comprehensive description of the burden and may prevent the underestimation of costs (2,7). However, it should be noted that overestimation of costs was also prevented by taking a conservative approach within the analysis (e.g., costs that could possibly be incurred by undiagnosed adults with ADHD were not quantified, such as healthcare costs derived from traffic accidents, fights, or drug consumption).
The results of previous studies that considered costs within four major domains (direct costs, indirect costs, education system costs, and justice system costs) closely resembled those reported in the present study. Accordingly, an annual cost per person of $US 20,538.95, of which 72% was attributed to work-related productivity costs, has been previously reported (7). Moreover, Sciberras et al (21) reported an annual cost per person of $US 15,664 of which 81% was attributed to work-related productivity costs. Though the latter estimated costs across the lifespan, the majority of costs were associated with adulthood (21). As the results of these studies, the estimated annual cost per patient in the present study was mainly attributed to work-related productivity costs within the economic domain (i.e., costs associated with mean wage reductions compared to non-ADHD, absenteeism, and presenteeism). However, only 45% of published studies on the economic burden of ADHD have captured indirect costs (i.e., work-related productivity) (7).
On the other hand, healthcare costs have been widely studied within economic burden studies (7). In this domain, the present study estimated an annual cost of €3,395.83 (21% of the total annual costs) and a one-time cost of €4,110.88 (52% of the total one-time costs) per patient diagnosed with ADHD. The latter included all medical consultations leading to diagnosis and those of the first-year post-diagnosis follow-up, contributing to the large one-time healthcare costs. However, these costs may be compensated with an appropriate treatment, which may have an impact on costs within other domains. Moreover, medication was estimated to be only 10% of the annual healthcare costs. This is particularly important for undiagnosed (i.e., untreated) adults, which accounts for 85% of adult patients with ADHD in Spain (4,13). In this regard, previous studies have shown that appropriate medication may reduce the risk of substance abuse (22,23), criminality (24), traffic accidents (25), and suicide attempts (26) in patients with ADHD, which may positively impact work-related productivity and other economic and/or legal issues.
However, the results of this study should be interpreted with caution given its limitations. First of all, the estimated burden of adult ADHD applies specifically to Spain and is therefore not representative of other countries. Within the healthcare domain, the large variability reported for the management of ADHD across regions of Spain may infer a large variability of costs as well. However, the present study did not include an interregion analysis of costs, which should be considered in future studies. Notwithstanding, a reasonable range for the consumption of healthcare resources was included in the sensitivity analysis to account for this variability. Moreover, healthcare costs incurred were mainly associated with ADHD follow-up and treatment and as such were only applied to adult patients with an ADHD diagnosis (0.5%) (12) for the estimation of total costs. Therefore, total costs incurred by adults with ADHD who are yet to be diagnosed and treated were underestimated, as the healthcare domain was not accounted for in these patients. Accordingly, future studies are encouraged to estimate the burden of adult ADHD before and after diagnosis, as it was not possible in the present study given the lack of scientific literature on the matter. Moreover, future studies should consider ADHD as a lifespan disorder in which any action taken during initial stages may drastically affect the course of the disorder and its burden (8).
Conclusions
The present study highlights the large burden that adult ADHD poses on the healthcare system and society at large. In contrast to childhood ADHD, symptoms in adulthood result in very serious consequences for the patients and society at large. The impact of ADHD encompasses almost every aspect of adult life, including social (e.g., substance abuse), work-related (e.g., productivity loss), and legal aspects (e.g., criminality). This is particularly important for undiagnosed patients with ADHD as appropriate treatments have shown positive results in these areas and may therefore reduce its associated socioeconomic burden. Accordingly, strategies that promote an early diagnosis and treatment should be implemented. The results of the present study can be used to inform policy and practice to help reduce the large burden of adult ADHD.
Acknowledgments
The authors thank Alexandra Ivanova from Vivactis Weber for the medical writing support. Medical writing support was funded by Takeda.
Disclosures
Conflicts of interest: FG declares no conflicts of interest. JAA, JB, MC, M Morales, and CM received consulting fees from Takeda as members of the Advisory Board. M Merino, PMH, and TML declare that they are employees of Vivactis Weber, an independent company that has received fees from Takeda for carrying out this study. JB received research grants and served as consultant, advisor, or speaker within the last 3 years for: AB-Biotics, Acadia Pharmaceuticals, Alkermes, Angelini, Ambrosetti-Angelini, Biogen, Casen Recordati, D&A Pharma, Exeltis, Gilead, Indivior, GW Pharmaceuticals, Janssen-Cilag, Jazz Pharmaceuticals, Lundbeck, Otsuka, Pfizer, Roche, Sage Therapeutics, Servier, Shire, Takeda. In addition, JB received research funding from the Spanish Ministry of Economy and Competitiveness—Centro de Investigación Biomedica en Red area de Salud Mental (CIBERSAM), and Instituto de Salud Carlos III, Spanish Ministry of Health. MC declares that the ADHD Program of the Department of Psychiatry, Hospital Universitari Vall d’Hebron, received unrestricted educational and research support from Eli Lilly and Co., Janssen-Cilag, Shire/Takeda, Rovi, Psious, and Laboratorios Rubió in the past two years. Moreover, MC received travel awards from Shire for participating in psychiatric meetings and acted as a consultant for Takeda.
Financial support: This study and the open access fee were funded by Takeda Farmaceutica España S.A.
Data availability: The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval: Not applicable.
Consent: Not applicable.
Author contributions: M Merino, PMH, and TML contributed to the study design, data collection, analysis, and interpretation. JAA, JB, MC, FG, M Morales, and CM contributed as members of the Advisory Board that provided expert appraisal for the study, including the economic model design, data collection and interpretation, and a critical review of the manuscript draft for important intellectual content. TML developed the original draft of the manuscript. M Merino and PMH critically revised the original draft. All authors approved the final submitted version of the manuscript.
References
- 1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, D.C.: American Psychiatric Association; 2013.
- 2. Kooij JJS, Bijlenga D, Salerno L, et al. Updated European Consensus Statement on diagnosis and treatment of adult ADHD. Eur Psychiatry. 2019;56(1):14-34. CrossRef PubMed
- 3. Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. 2015;56(3):345-365. Online CrossRef PubMed
- 4. Fayyad J, Sampson NA, Hwang I, et al; WHO World Mental Health Survey Collaborators. The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. Atten Defic Hyperact Disord. 2017;9(1):47-65. Online CrossRef PubMed
- 5. Holst Y, Thorell LB. Functional impairments among adults with ADHD: a comparison with adults with other psychiatric disorders and links to executive deficits. Appl Neuropsychol Adult. 2020;27(3):243-255. Online CrossRef PubMed
- 6. Chhibber A, Watanabe AH, Chaisai C, Veettil S, Chaiyakunapruk N. PMH20 economic burden of attention-deficit/hyperactivity disorder (ADHD): a global systematic review. Value Health. 2020;23:S203. Online CrossRef
- 7. Chhibber A, Watanabe AH, Chaisai C, Veettil SK, Chaiyakunapruk N. Global economic burden of attention-deficit/hyperactivity disorder: a systematic review. PharmacoEconomics. 2021;39(4):399-420. CrossRef PubMed
- 8. Franke B, Michelini G, Asherson P, et al. Live fast, die young? A review on the developmental trajectories of ADHD across the lifespan. Eur Neuropsychopharmacol. 2018;28(10):1059-1088. Online CrossRef PubMed
- 9. Ginsberg Y, Quintero J, Anand E, Casillas M, Upadhyaya HP. Underdiagnosis of attention-deficit/hyperactivity disorder in adult patients: a review of the literature. Prim Care Companion CNS Disord. 2014;16(3):PCC.13r01600. CrossRef PubMed
- 10. Du Rietz E, Jangmo A, Kuja-Halkola R, et al. Trajectories of healthcare utilization and costs of psychiatric and somatic multimorbidity in adults with childhood ADHD: a prospective register-based study. J Child Psychol Psychiatry. 2020 Sep;61(9):959-968. CrossRef PubMed
- 11. Quintero J, Ramos-Quiroga JA, Sebastián JS, et al. Health care and societal costs of the management of children and adolescents with attention-deficit/hyperactivity disorder in Spain: a descriptive analysis. BMC Psychiatry. 2018;18(1):40. Online CrossRef PubMed
- 12. Ramos-Quiroga JA, Targhetta M, Gasche D, Rubio M, Perulero N. PND71 epidemiology of attention deficit hyperactivity disorders in Spain based on real-world data. Value Health. 2019;22:S750. Online CrossRef
- 13. Instituto Nacional de Estadística. Estadística Continua de Población. Datos provisionales a 1 de enero de 2019. [Internet]. INE Instituto Nacional de Estadística 2019. Online. Accessed October 2023.
- 14. Ramos-Quiroga JA, Tang JP, Solozabal M, Prado AD, Miñarro C, Callejo-Velasco D. PND124 a real-world data study to analyse the pharmacological treatment of attention deficit hyperactivity disorder in Spain. Value Health. 2019;22:S760. Online CrossRef
- 15. Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). Elvanse. Ficha técnica o resumen de las características del producto. Online. Accessed October 2023.
- 16. Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). Medikinet. Ficha técnica o resumen de las características del producto. Online. Accessed October 2023.
- 17. Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). Strattera. Ficha técnica o resumen de las características del producto. Online. Accessed October 2023.
- 18. Consejo General de Colegios Oficiales de Farmacéuticos. BOTPLUS [Internet]. BOTPLUS 2020 Online. Accessed October 2023.
- 19. Instituto Nacional de Estadística. Índice de Precios de Consumo. Base 2016. Medias anuales. Índices nacionales: general y de grupos ECOICOP Online. Accessed October 2023.
- 20. Shemilt I, James T, Marcello M. A web-based tool for adjusting costs to a specific target currency and price year. Evid Policy. 2010;6(1):51-59. Online CrossRef
- 21. Sciberras E, Streatfeild J, Ceccato T, et al. Social and economic costs of attention-deficit/hyperactivity disorder across the lifespan. J Atten Disord. 2020;108705472096182 Online PubMed
- 22. Quinn PD, Chang Z, Hur K, et al. ADHD medication and substance-related problems. Am J Psychiatry. 2017;174(9):877-885. Online CrossRef PubMed
- 23. Chang Z, Lichtenstein P, Halldner L, et al. Stimulant ADHD medication and risk for substance abuse. J Child Psychol Psychiatry. 2014;55(8):878-885. Online CrossRef PubMed
- 24. Lichtenstein P, Larsson H, Zetterqvist J, et al. Medication for attention deficit-hyperactivity disorder and criminality. N Engl J Med. 2013;368(8):776. Online PubMed
- 25. Chang Z, Lichtenstein P, D’Onofrio BM, Sjölander A, Larsson H. Serious transport accidents in adults with ADHD, and the effect of medication: a population based study. JAMA Psychiatry. 2014;71(3):319-325. Online CrossRef PubMed
- 26. Chen Q, Sjölander A, Runeson B, D’Onofrio BM, Lichtenstein P, Larsson H. Drug treatment for attention-deficit/hyperactivity disorder and suicidal behaviour: register based study. BMJ. 2014;348(jun18 18):g3769. Online CrossRef PubMed
- 27. aci H, Asherson P, Donfrancesco R, et al. Daily life impairments associated with childhood/adolescent attention-deficit/hyperactivity disorder as recalled by adults: results from the European Lifetime Impairment Survey. CNS Spectr. 2015;20(2):112-121. CrossRef PubMed
- 28. Able SL, Haynes V, Hong J. Diagnosis, treatment, and burden of illness among adults with attention-deficit/hyperactivity disorder in Europe. Pragmat Obs Res. 2014;5:21-33. Online CrossRef PubMed
- 29. Ministerio de Sanidad, Consumo y Bienestar Social. Consulta Interactiva del SNS. Registro de Actividad de Atención Especializada RAE-CMBD. Coste medio APR. 2017. Públicos-SNS. Categoría CSS CIE10 244-Otras lesiones y afecciones debidas a causas externas. [Internet]. Portal Estadístico 2020 Online (Accessed October 2023)
- 30. Mosquera Nogueira J, Rodríguez-Míguez E. Intangible costs of alcohol dependence from the perspective of patients and their relatives: a contingent valuation study. Adicciones. 2018;30(2):111-122. CrossRef PubMed
- 31. Trapero‐Bertran M, Leidl R, Muñoz C, et al. Estimates of costs for modelling return on investment from smoking cessation interventions. Addiction [Internet] 2018 [cited 2020 Aug 19];113(Suppl 1):32–41. Online CrossRef
- 32. Piñeiro-Dieguez B, Balanzá-Martínez V, García-García P, Soler-López B; CAT Study Group. Psychiatric comorbidity at the time of diagnosis in adults with ADHD: the CAT Study. J Atten Disord. 2016;20(12):1066-1075. CrossRef PubMed
- 33. Oliva J, Rivera B. Los costes sociales del consumo de drogas ilegales en la Comunidad de Galicia. Presupuesto y Gasto Público. 2006;44:105-131. Online. Accessed October 2023.
- 34. Herranz Ramia Abogados. ¿Cuánto cuesta un divorcio actualmente en España? 2020. [Internet]. Herranz Ramia 2018 Online. Accessed October 2023.
- 35. Brod M, Pohlman B, Lasser R, Hodgkins P. Comparison of the burden of illness for adults with ADHD across seven countries: a qualitative study. Health Qual Life Outcomes. 2012;10(1):47. CrossRef PubMed
- 36. Johnson SM. The practice of emotionally focused couple therapy: creating connection. Routledge; 2019. CrossRef
- 37. Ljung T, Chen Q, Lichtenstein P, Larsson H. Common etiological factors of attention-deficit/hyperactivity disorder and suicidal behavior: a population-based study in Sweden. JAMA Psychiatry. 2014;71(8):958-964. CrossRef PubMed
- 38. Alfonso-Sánchez JL, Martin-Moreno JM, Martinez IM, Martinez AA. Epidemiological study and cost analysis of suicide in Spain: over 100 years of evolution. Arch Suicide Res. 2020;24(sup2):S356-S369. CrossRef PubMed
- 39. Hartge J, Toledo P. Attention Deficit Hyperactivity Disorder (ADHD) and its comorbid mental disorders: an evaluation of their labor market outcomes. J Ment Health Policy Econ. 2018;21(3):105-121. PubMed
- 40. Instituto Nacional de Estadística. Encuestas de estructura salarial. Ganancia media anual por trabajador. [Internet]. INE2017 Online. Accessed October 2023.
- 41. Daley D, Jacobsen RH, Lange AM, Sørensen A, Walldorf J. The economic burden of adult attention deficit hyperactivity disorder: a sibling comparison cost analysis. Eur Psychiatry. 2019;61:41-48. Online CrossRef PubMed
- 42. Instituto Nacional de Estadística. Encuesta Anual de Estructura Salarial 2016. Online. Accessed October 2023.
- 43. Blasco de Luna FJ, Barceló Larran D, Blázquez Agudo EM, et al. VIII Informe Adecco sobre absentismo. [Internet] The Adecco Group Institute; 2019, Available from Online. Accessed August 21, 2020.
- 44. de España B. Encuesta Financiera de las Familias (EFF) 2017: métodos, resultados y cambios desde 2014 [Internet]. Banco de España; 2020 Online. Accessed October 2023.
- 45. Multas y accidentes de tráfico, ¿cuáles son las causas principales? Online. Accessed October 2023.
- 46. Barkley RA, Murphy KR, Dupaul GI, Bush T. Driving in young adults with attention deficit hyperactivity disorder: knowledge, performance, adverse outcomes, and the role of executive functioning. J Int Neuropsychol Soc. 2002;8(5):655-672. CrossRef PubMed
- 47. BOE núm. 85. Ley 6/2014, de 7 de abril, por la que se modifica el texto articulado de la Ley sobre Tráfico, Circulación de Vehículos a Motor y Seguridad Vial, aprobado por el Real Decreto Legislativo 339/1990, de 2 de marzo. Online
- 48. Inspección Técnica de Vehículos. Cómo recuperar los puntos del carnet de conducir [Internet]. ITV.com.es 2018 Online. Accessed October 2023.
- 49. Arpem. El precio medio de un seguro de coche en España fue de 479€ en 2019 Online. Accessed October 2023
- 50. Acierto. El historial de siniestralidad del conductor, ¿qué es? Online. Accessed October 2023.
- 51. Biederman J, Faraone SV, Spencer TJ, Mick E, Monuteaux MC, Aleardi M. Functional impairments in adults with self-reports of diagnosed ADHD: a controlled study of 1001 adults in the community. J Clin Psychiatry. 2006;67(4):524-540. Online CrossRef PubMed
- 52. Mannuzza S, Klein RG, Moulton JL III. Lifetime criminality among boys with attention deficit hyperactivity disorder: a prospective follow-up study into adulthood using official arrest records. Psychiatry Res. 2008;160(3):237-246. Online CrossRef PubMed
- 53. Francisco Sevilla Cáceres. ¿Cuanto tengo que pagarle a mi abogado? Online. Accessed October 2023.
- 54. Aebi MF, Tiago MM. SPACE I - 2019 - Council of Europe Annual Penal Statistics: Prison populations. [Internet] Council of Europe; 2020, Available from Online. Accessed August 21, 2020.