|
Arch Physioter 2025; 15: 59-68 ISSN 2057-0082 | DOI: 10.33393/aop.2025.3301 ORIGINAL RESEARCH ARTICLE |
Mim-pong: a serious game for assessment and treatment of the lower limb in hemiparetic stroke patients
Fernando LF Eichinger![]() 1, Fabrício Noveletto
1, Fabrício Noveletto![]() 2, Susana C Domenech
2, Susana C Domenech![]() 3, Thierry Moulin
3, Thierry Moulin![]() 4, Yoshimasa Sagawa
4, Yoshimasa Sagawa![]() 4, Antonio V Soares
4, Antonio V Soares![]() 1,4
1,4
ABSTRACT
Introduction: The motor impairment evidenced post-stroke results in limitations to performing activities of daily living (ADL), especially when it involves locomotion. The Serious Games (SG) are an interesting therapeutic option, as they allow the performance of exercises according to stroke treatment guidelines. However, there is little research exploring the evaluation potential of SG. This study aimed to evaluate the possible metric properties of the mim-pong SG in addition to the therapeutic effects.
Methods: Twenty-four hemiparetic stroke patients were divided into two non-randomized groups: the experimental group (EG) (n = 16) and the control group (CG) (n = 8). Participants were evaluated in terms of motor impairment (lower limb), muscle strength (MS), motor control, and functional mobility.
Results: The significant correlations observed between the score generated by the SG and clinical variables in both groups are highlighted, especially with MS (rho = 0.62-0.66; p = 0.000, and rho = 0.67-0.71; p = 0.002-0.005, for the experimental and CGs, respectively) and motor function of the lower limb for the EG (rho = 0.41, p = 0.018). In addition, the results indicated improvements in all variables in the EG, with superiority over the CG.
Conclusions: This study showed that the mim-pong serious game could be considered a potential resource for the assessment and treatment of hemiparetic stroke patients.
Keywords: Exercise therapy, Hemiparesis, Lower extremity, Rehabilitation, Serious games, Stroke
Received: September 12, 2024
Accepted: February 25, 2025
Published online: March 24, 2025
Clinical Trial Protocol number: Brazilian Registry of Clinical Trials (RBR-2MF595).
Corresponding author:
Antonio V Soares
email: antonio.vinicius@univille
Archives of Physiotherapy - ISSN 2057-0082 - www.archivesofphysiotherapy.com
© 2025 The Authors. This article is published by AboutScience and licensed under Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0).
Commercial use is not permitted and is subject to Publisher’s permissions. Full information is available at www.aboutscience.eu
What is already known about this topic:
- Serious Games represent a new technology that addresses the main requirements of rehabilitation: attention, motivation and training (repetition).
What does the study add:
- The study presents an SG developed for post-stroke rehabilitation. The results showed the therapeutic effects and potential metric properties of this technology.
Introduction
Stroke is the second leading cause of death and the main cause of long-term disability worldwide (1,2). According to the World Health Organization (WHO), more than 15 million people suffer from a stroke annually (3). Among the clinical aspects, motor dysfunction is the most common and disabling complication of patients, present in approximately 80% of cases (4,5).
Hemiparesis is the typical post-stroke dysfunction, described as partial loss of muscle strength (MS) in the contralateral hemibody to the brain injury (6). Impairment in the lower limbs, especially in the quadriceps femoris (QF) and the hamstrings (HS) muscle groups, has a great impact on the functional independence of patients, as it affects locomotor skills and increases the risk of falls in most patients (7).
The motor impairment evidenced after stroke results in limitations in performing activities of daily living (ADLs) (8), especially when it involves the lower limb. Thus, there are often difficulties in performing basic and essential tasks such as walking, sitting, standing up, and going up and down stairs, which significantly reduces quality of life (9). In this context, stroke rehabilitation plays a key role, especially if started early (10).
Motor function recovery is a major rehabilitation target for patients with stroke (11), as it allows the optimization of residual capacities to improve functionality, reflecting greater participation in social activities (5,10). In this direction, the recovery of the lower limb can improve gait, which is one of the main objectives of these patients (12).
There are several therapeutic strategies aimed at lower limb rehabilitation, including conventional kinesiotherapy based on mobilization, stretching, and strengthening exercises (13). Although evidence indicates the beneficial effects of this type of therapy, there are important limitations that must be considered, especially those related to repetitiveness, boredom, and monotony, as they can result in difficulty adhering to treatment (14–16).
Seeking to provide a more engaging and motivating experience for patients and overcoming the limitations of conventional therapy, the use of games as a therapeutic resource for patients with stroke has increased in recent years (17). From this perspective, Serious Games (SG) stand out, which are games created in a virtual environment with specific objectives, allowing customization according to the patient’s limitations while combining physical training and motor rehabilitation without losing the common motivational focus of an electronic game (18–20).
SG is an interesting therapeutic option because it allows for the performance of exercises in accordance with the guidelines for stroke treatment, which recommend task-oriented practice with intensity and repetitiveness, adding a higher level of attention and motivation during sessions (13,18). The low cost, accessibility, and portability of SG have made them invaluable for patient assessment and treatment (21).
The effectiveness of SG in stroke rehabilitation has already been proven, especially in approaches aimed at the upper limb (17,18). Regarding application to the lower limb, there are still few studies on effectiveness, and publications aimed at the potential for evaluating these resources are even more uncommon.
Due to the limited research exploring the potential of SG for assessment, the aim of this study was to verify whether the mim-Pong SG developed for the evaluation and treatment of lower limbs in stroke patients has metric properties.
Materials and methods
Design and context of the study
This Non-Randomized Controlled Clinical Trial involved patients with stroke. The study was carried out at the Center of Research in Neurorehabilitation at the Neurology Outpatient Clinic of the Guilherme Guimbala College, Joinville, Santa Catarina, Brazil.
Participants
The inclusion criteria were patients with subacute or chronic hemiparesis due to stroke (injury time ≥3 months), clinically stable, and able to walk independently. The exclusion criteria were hemiparesis due to other diseases, symmetric bilateral motor impairment, severe visual and/or auditory impairment, uncooperative patients and/or with severe cognitive deficits, and patients who were performing or who performed (in the last 3 months) any other type of rehabilitation for the trunk and/or lower limbs.
This study was approved by the Ethics Committee for Research with Humans (CAAE 56995816.6.0000.0118), by the Brazilian Registry of Clinical Trials (RBR-2MF595), and the procedures were in accordance with the Helsinki Declaration.
Evaluations
The evaluations and instruments used were chosen according to the International Classification of Functioning, Disability, and Health (ICF) domains, developed by the WHO in 2004.
– Anthropometric digital scale and stadiometer to measure body mass and height, respectively.
– Fugl-Meyer Assessment Scale (FMAS) to measure the level of motor impairment in the patients (22). Only the section for motor evaluation of the lower limb was used, which includes the analysis of reflex activity, synergic muscular action in flexion and extension, and movements with and without synergy.
– Mini-Mental State Examination (MMSE) to assess the cognitive level of patients. This instrument was used only for patient screening following the cut-off points related to schooling (23).
– Mim-Pong SG: for assessment of the performance during the game, MS and motor control (MC). Mim-pong SG was also used for the training of patients. This game operates by means of a system based on a load cell (IWM brand, single point load type, Brazil, capacity of 589 N, accuracy <0.017% – full scale).
The score for assessing the patient’s performance during the training considers the aspects related to the gameplay and is obtained through the equation proposed previously by this study’s research group (19). This SG has simple visual aspects that focus the patient on hitting the ball using a “racket” (Fig. 1). Rackets move simultaneously on the screen’s vertical sides based on the strength applied to the load cell, which can be calibrated individually with the evaluation of the maximal voluntary isometric contraction (MVIC) of each muscle group in each session. However, when no strength is applied, the rackets stay still at the bottom of the screen. The upper limit of the rackets (at the top of the screen) is based on the MVIC of each subject. The horizontal walls bounce the ball back. To improve the challenge, game parameters can be adjusted: for example, the racket size, ball size, ball speed, and duration of the match.
Two muscle groups of the lower limb were evaluated: QF and HS. For operation, specific software and hardware were developed. The hardware used the signal obtained from the load cells as a dynamometry (Fig. 2).
For the evaluation of MS, the load cell was coupled to a device that allows the adjustment and positioning of the region to be worked, acting as a hand-held dynamometer for measuring any muscle group (19). The software enables the configuration of hardware-related parameters, calibration for acquisition initialization, real-time visualization of the captured signal, and recording of acquisition data.
For evaluation and training with the mim-Pong SG, a leg extensor apparatus was prepared and adapted with a load cell, which was coupled to the chair and allowed to assess the strength bilaterally of the muscle groups previously mentioned (QF and HS). Both the patient and device position depend on the muscular group analyzed as follows. For the QF, the patient sits in the chair with the trunk supported by the backrest, legs hanging, hip at 110º of flexion relative to the trunk, and knees flexed at 90º (7). The sensor is placed perpendicular to the distal third of the leg (just above the malleolar region) on the anterior face. For the HS test, the patient is positioned in the chair as in the QF test, but with knees flexed at 60º (24), and the sensor is placed perpendicular to the distal third of the leg on the posterior face (19).
For the evaluation of MS, three measures were performed bilaterally of each muscle group in the MVIC for 5 seconds (24), with an interval of 1 minute between each measurement. All evaluations (QF and HS) were conducted on alternate days, with a minimum interval of 24 hours, and performed by the same examiners. The patient was instructed to perform as much force as possible from a green signal projected on the screen, which indicated the beginning of the test, and this force should be maintained until the green color disappears, indicating the end of the test. After the MS measurement, the patient had a rest period of 2 minutes to then carry out the MC assessment protocol.
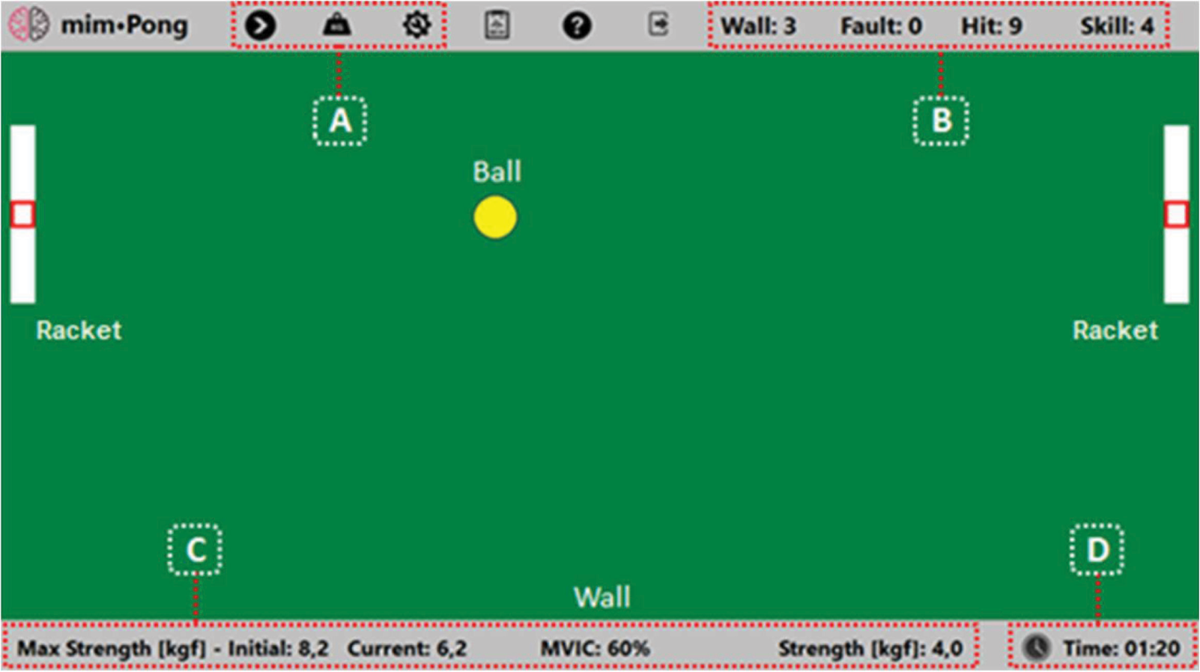
FIGURE 1 - The mim-pong SG main screen.
A) Game control and settings; B) Game score components; C) Muscular strength data; D) Game session time elapsed. The figure was created by (7).
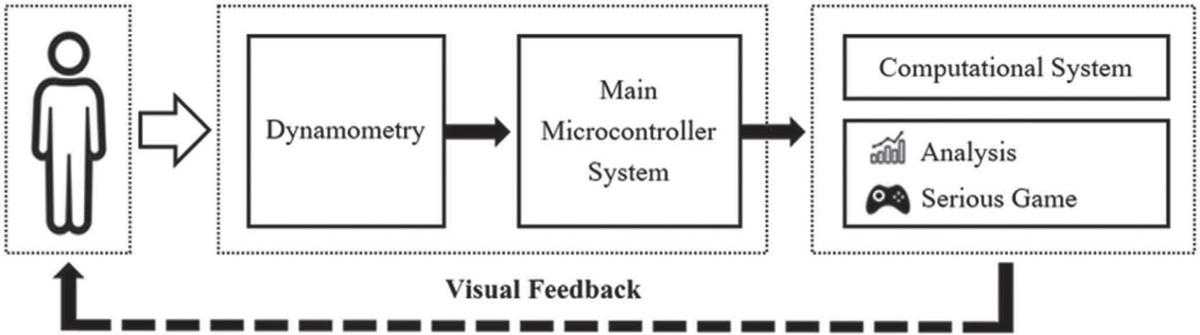
FIGURE 2 - General diagram illustrating the basic units of the system used for the evaluation and treatment of patients.
The assessment of patients’ MC consisted of a task in which the goal was to hit a ball at 5 different levels, from 1 to 5 (Figure 3). These levels are associated with the MVIC obtained during the MS. At level 1, the patient should produce strength equivalent to 20% MVIC to hit the ball in the racquet’s center. Levels 2 to 5 represent the percentages of 40, 60, 80, and 100% MVIC, respectively. The rationale for these different levels of strength is that most tasks performed in daily life do not require the use of maximum strength for their performance (25,26). The ball moved in a straight line from the left side of the screen to the right side, where the racket was located at different levels, representing the percentages of the MVIC. One ball leaves every 10 seconds, starting with the lower strength level (20% of the MVIC) up to the maximum level (100% of the MVIC). At the end of the test, the mim-pong SG provides an evaluation score that indicates the patient’s MC. The maximum score in the evaluation mode is 100. The patient’s MC score was calculated according to the equation created by (19), which considers the position of hitting the racket as well as the effort required to hit the ball at each level of the assessment mode. Lower levels require less MS and, therefore, represent a smaller weight in the score’s composition.
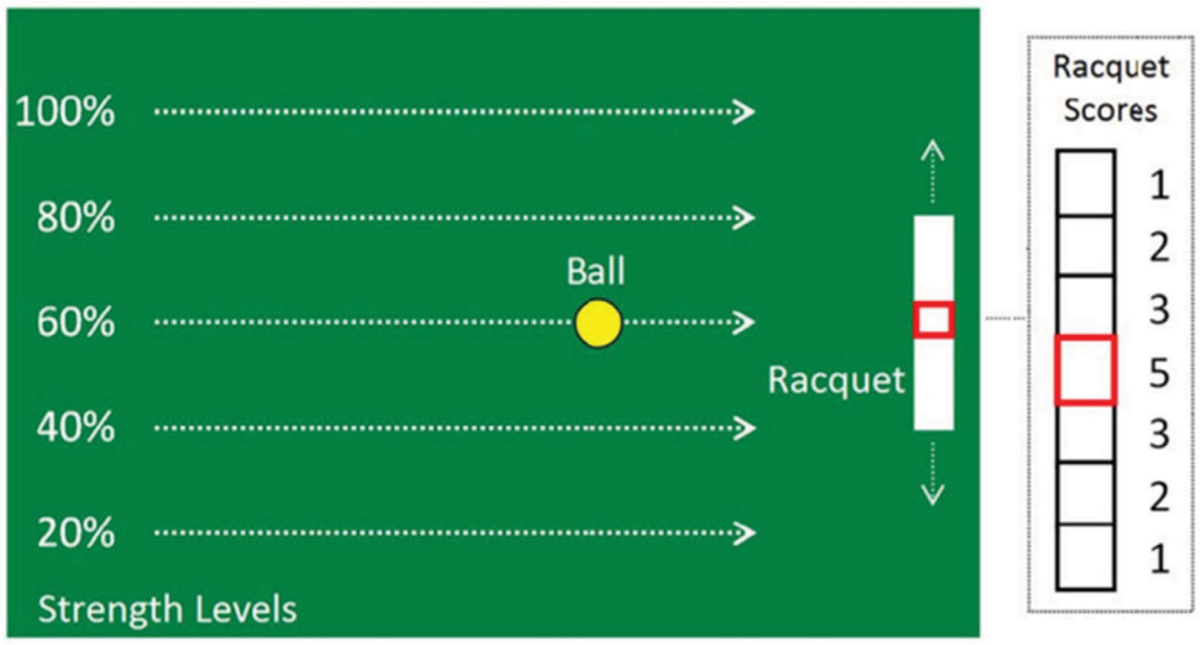
FIGURE 3 - Assessment protocol for motor control.
The hit score values on the racquet are shown zoomed on the right side. The closer to the racquet’s center, the higher the score. The score is equal to zero if the ball does not hit the racquet. This figure was created by (19).
– Timed Up and Go (TUG) Test: to assess functional mobility by measuring the time taken to perform the proposed task (7).
Interventions
After the evaluation phase, the patients of both groups were submitted to the same treatment period, 10 consecutive weeks, with two sessions per week on alternate days for a total of 10 hours of training (each training session lasted 30 minutes). The participants were divided into two non-randomized groups: the experimental group (EG 16 patients) and the control group (CG 8 patients). Due to operational constraints related to the researchers’ availability to conduct the experiment, the CG consisted of only 8 patients.
The EG received a rehabilitation program for the paretic lower limb based on exercises using the mim-pong SG. This exercise program (as described in assessing the patient’s performance during the training) was divided into two phases with 10 sessions: phase 1 (using 60% of the MVIC) and phase 2 (using 80% of the MVIC). These percentage values fulfill the guidelines of resistance exercises for patients with stroke (27). The same configuration of the game (racket size, ball size, and ball speed) was standardized for all patients. In each session, the passive mobilization of the paretic side was performed for a period of 10 minutes, after which the training was started. An SG calibration was always performed by measuring the MVIC, and after obtaining this data, the exercise was started with the patient. Each session was composed of three sets of 2 minutes with a 1-minute break between each set for rest for each paretic muscle group (QF and HS). The sessions always started with the strengthening of the QF, and then the exercises for HS were performed after.
The CG received a rehabilitation program based on conventional kinesiotherapy (passive mobilization and stretching exercises). The sessions performed with this group also lasted 30 minutes. Initially, 10 minutes of passive mobilization were performed. This was followed by 20 minutes of strengthening exercises using manually resisted active movements conducted by the researcher, as load tolerance varied among patients. It is important to note that, as in the EG, training was performed exclusively on the paretic side.
Evaluations
The evaluations were carried out three times in the week prior to initiating the rehabilitation and three times in the week following the end of the program. The arithmetic mean resulting from these three evaluations was used for further analysis.
Statistical analysis
The data was analyzed using IBM SPSS for Windows, version 20.0. A per-protocol analysis was performed. Descriptive statistics (mean, median, standard deviation, and frequency distribution with absolute and percentage values) were used for participant characterization. Data normality was verified by the Shapiro-Wilk test and the homogeneity of variances by the Levene test. The one-way ANOVA and Tukey’s multiple comparison tests were used to verify the effect of the group (EG vs CG) and the effect of the condition (pre- and post-intervention) on the studied variables. The variables that did not meet the assumptions for the ANOVA underwent two-group comparison tests: the Mann-Whitney U test when comparing the EG and CG or the Wilcoxon rank-sum test when comparing pre- and post-intervention conditions. Effect Size (ES) was calculated to evaluate whether the observed differences corresponded to clinically significant effects. For parametric data, ES values <0.2, 0.2-0.8, and ≥0.8 were considered small, medium, and large, respectively. For non-parametric data, ES values were <0.1, 0.2-0.5, and ≥0.5. The Spearman correlation test was used to evaluate the potential metric properties of the mim-pong SG. The correlation values <0.3, 0.2-0.5, and >0.5 were considered small, medium, and large, respectively. A significance level of 0.05 was used for all tests.
Results
Table 1 presents the sociodemographic, clinical, and anthropometric characterization of the participants of the EG and CG. Twenty-four patients (12 males and 12 females; mean (SD) age of 58 (10) years old; mean (SD) time since stroke of 16.8 (19.6) months) participated in this study. In both groups, a predominance of ischemic stroke was observed (EG = 80% and CG = 62.5%), and there was a prevalence of hemiparesis on the left side of the body. All patients completed all stages of the experiment. A comparison of the sociodemographic, clinical, and anthropometric variables between the EG and the CG in the pre-intervention period revealed that there were no statistically significant differences between groups in any of the variables studied.
Table 2 shows the results of the correlation analyses between the scores obtained with mim-pong SG and the other variables studied, which were used to examine the potential metric properties of the SG. The score provided by the SG was significantly correlated with MS in both the QF and HS (large correlation) in both groups. A moderate and significant correlation between the HS score and the TUG was observed only in the CG, while a medium and significant correlation between the QF score and the FMAS was found only in the EG.
| Characteristics | EG (n = 16) | CG (n = 8) | p-value |
|---|---|---|---|
| Sex (female; f, %) | 8.50% | 4.50% | – |
| Age (years) | 56.8 (10.8) | 59.8 (9.8) | 0.515a |
| BMI (kg/m2) | 29.1 (7.8) | 28.3 (5.8) | 0.796a |
| Hemiparesis (left; f, %) | 9.56% | 4.50% | – |
| Stroke time (months) | 19.3 (23.1) | 13.8 (12.3) | 0,666b |
| Phase of the stroke (chronic; f, %) | 11.67% | 5.62% | – |
| Type of the stroke (Ischemic; f, %) | 13.81% | 5.62% | – |
Significance level p < 0,05; p-value: probability of significance obtained by the independent t-test (a) or by the Mann-Whitney U test (b). EG: experimental group; CG: control group; BMI: body mass index; n: total sample; f: absolute frequency.
| Mim-pong scores | ||||||||
|---|---|---|---|---|---|---|---|---|
| EG | CG | |||||||
| Variables | Score QF | Score HS | Score QF | Score HS | ||||
| rho | p | rho | p | rho | p | rho | p | |
| QF strength* | 0.62 | 0.000 | 0.29 | 0.109 | 0.67 | 0.005 | 0.35 | 0.184 |
| Hamstrings strength* | 0.66 | 0.000 | 0.41 | 0.019 | 0.71 | 0.002 | 0.74 | 0.001 |
| FMAS | 0.41 | 0.018 | 0.34 | 0.061 | 0.35 | 0.185 | 0.45 | 0.082 |
| Timed up and go | −0.29 | 0.105 | −0.33 | 0.065 | −0.39 | 0.138 | −0.54 | 0.032 |
rho, Spearman correlation; p, Significance level <0.05; *only paretic side; Numbers in red indicate statistical significance.
Regarding the comparison between groups (Table 3), in the pre-intervention condition, no statistically significant differences were observed in any variable.
Regarding the comparison between groups (Table 3), in the post-intervention condition, statistically significant differences were observed for QF MC of the paretic (p = 0.001) and nonparetic (p = 0.029) sides and for HS MC of the nonparetic sides (p = 0.029).
Comparisons between pre- and post-intervention conditions in the EG showed statistically significant differences for all the variables studied except the QF MS of the non-paretic side (p = 0.093).
Comparisons between pre- and post-intervention conditions in the CG showed statistically significant differences only for QF MC (p = 0.003) and HS MC (p = 0.006).
Discussion
There are already some studies indicating the potential benefits of SG for the rehabilitation of patients with stroke. Our study aimed to explore the possible metric properties of the mim-pong SG, as well as to evaluate the therapeutic effects derived from an exercise program using this resource.
The analysis of the metric properties of the game (Table 2) indicated that the mim-pong SG can be used not only for treatment but also as an assessment tool for patients. The highest correlations observed (large and significant) were between the scores generated by the SG and MS variables in the QF and HS in both groups. One hypothesis to explain this finding is related to the elements that compose the formula for calculating the game score, with MS being one of the clinical elements considered. Therefore, as patients show improvement in their MS levels, the score also tends to be higher.
| Group | Pre | Post | p-value (pre vs post) |
ES | p-value (EG vs CG)* |
|
|---|---|---|---|---|---|---|
| Paretic side | ||||||
| QF MS (kgf)b | Exp. | 14.8 (6.6) | 21.2 (11.6) | 0.000 | 0.6 | 0.268 |
| Cont. | 14.7 (11.9) | 15.4 (12.0) | 0.185 | 0.1 | ||
| Hamstrings MS (kgf)a | Exp. | 5.4 (3.0) | 10.2 (4.3) | 0.000 | 1.3 | 0.322 |
| Cont. | 7.1 (6.3) | 8.1 (6.0) | 0.069 | 0.5 | ||
| QF motor control (score)b | Exp. | 67.8 (18.7) | 87.8 (12.8) | 0.000 | 0.6 | 0.001 |
| Cont. | 52.4 (19.9) | 65.0 (17.1) | 0.003 | 0.7 | ||
| Hamstrings motor control (score)a | Exp. | 54.3 (21.8) | 78.9 (16.6) | 0.000 | 1.3 | 0.220 |
| Cont. | 51.3 (27.7) | 64.8 (25.2) | 0.006 | 0.5 | ||
| Nonparetic side | ||||||
| QF MS (kgf)b | Exp. | 24.3 (7.3) | 27.5 (10.9) | 0.093 | 0.3 | 0.462 |
| Cont. | 23.9 (8.8) | 24.2 (10.0) | 0.761 | 0.1 | ||
| Hamstrings MS (kgf)a | Exp. | 11.7 (4.2) | 15.2 (5.2) | 0.000 | 0.8 | 0.342 |
| Cont. | 12.8 (7.0) | 13.1 (4.4) | 0.744 | 0.1 | ||
| QF motor control (score)b | Exp. | 78.8 (11.7) | 87.6 (4.7) | 0.004 | 0.5 | 0.029 |
| Cont. | 65.6 (16.1) | 74.3 (13.7) | 0.142 | 0.5 | ||
| Hamstrings motor control (score)a | Exp. | 69.9 (14.2) | 82.3 (12.6) | 0.001 | 0.8 | 0.029 |
| Cont. | 64.8 (20.9) | 69.3 (13.4) | 0.407 | 0.3 | ||
| FMASb | Exp. | 21.1 (4.8) | 24.3 (3.3) | 0.000 | 0.6 | 0.877 |
| Cont. | 22.4 (6.3) | 23.9 (4.6) | 0.068 | 0.5 | ||
| TUG test (s)b | Exp. | 22.5 (20.4) | 18.4 (15.7) | 0,001 | 0.6 | 0.668 |
| Cont. | 33.3 (28.4) | 28.9 (22.0) | 0.247 | 0.4 |
Significance level p < 0.05; p-value: probability of significance obtained by the paired t-test (a) or by the Wilcoxon signed-rank test (b); ES: effect size; EG: experimental group; CG: control group. *comparison post-intervention
Among the important variables in resistance training are intensity and the number of repetitions performed during an exercise (28). The utilized SG provided an intense training session with a high number of exercise repetitions, which contributed to the observed improvements. In this sense, training with adequate intensity and repeatability can improve MC in the lower limbs, in addition to increasing MS (29).
In the EG, a moderate and significant correlation was also found between the score and the FMAS, which evaluates motor impairment in patients. This scale includes the analysis of various factors related to motor function, including synergistic muscle action in flexion and extension (22), which may explain the findings. In the CG, a moderate and significant correlation was observed between the score and functional mobility. This is supported by a study involving 21 stroke patients. It was found that MC deficits rather than MS deficits predict functional impairments in mobility (30). Therefore, it is recommended to prioritize rehabilitation interventions aimed at improving MC as they may yield better functional outcomes in these patients. In fact, most daily activities do not require maximum levels of MS (25), which makes the mim-pong SG even more valuable as it takes this factor into account by requiring patients to adjust to various levels of contraction, thus promoting improvements in MC.
In commercial games frequently used in rehabilitation, there is no concern while designing game scores toward the patient’s clinical monitoring (16). Thus, as already mentioned, the SG scores were related to important clinical variables (MS, motor impairment, and functional mobility), indicating that the mim-pong SG can contribute not only to the treatment but also to the assessment of patients, being a measure of therapeutic progress.
The muscle strengthening programs based on SG should include elements described as essential in rehabilitation, for example, intensity, repetitiveness, and task-oriented training (19). Thus, they become effective for the rehabilitation of these patients and contribute to a more attractive and motivational therapeutic process, overcoming the limitations often evidenced in conventional therapies (13,18,19). It is believed that motivated behaviors lead to improved performance, and thus, motivation has been shown to be an important element in the association between cognition and motor performance, playing a crucial role in rehabilitation outcomes (31).
In this study, the exercise program with the mim-pong SG resulted in significant improvements in all variables analyzed in the EG. In the group receiving conventional treatment, significant improvements were observed only in the MC of the QF and the HS in the paretic limb.
The hemiparesis present after a stroke is related to high rates of functional disability, evidenced by the difficulty in performing ADL (8,11,32). Muscle weakness in the lower limbs limits fundamental activities such as walking, sitting, standing, and climbing stairs, which significantly impacts quality of life (6,33). In general, the participants of this study had an important hemiparesis in both muscle groups, but more evident in the HS. In the EG, 39.3% lower QF strength and 53.0% lower HS strength were observed than in the non-paretic side. In the CG, much lower strength levels were also observed on the paretic side, 38.5% in the QF and 44.5% in the HS.
An important clinical result of this study was the MS gain. In the EG, significant gains were obtained on the paretic side with a large ES for the HS (p = 0.000, ES = 1.3) and moderate ES for the QF (p = 0.003, ES = 0.6). The EG also showed an improvement in the non-paretic side’s MS, with statistically significant results and a large ES for the QF (p = 0.004, ES = 0.5) and the HS (p = 0.001, ES = 0.8). In the CG, there were no significant improvements, and the ES was small for the QF and moderate for the HS on the paretic side. Although for MS, no statistically significant differences were found when comparing between groups in the post-experimental period, it is possible to see that the effects were greater in the EG. In recent years, there has been an increase in studies attempting to detect the so-called minimum clinically important difference (MCID), defined by Jaeschke et al. (34) as the “smallest difference in scores in the domain of interest that patients perceive as beneficial and that would require, in the absence of troublesome side effects and excessive costs, a change in patient management.” In this sense, the literature indicates that for MS in the QF in individuals with limited physical activity, an MCID of 3.0 kgf is considered (35). Thus, comparing the means between the groups, indeed, the EG obtained greater improvement (difference of 5.7), while the CG did not reach the MCID. In the MS of the HS, a greater difference was also noted in the EG compared to the CG (difference of 3.8).
Systematic reviews show that resistance training has been beneficial in patients with stroke for improving lower limb MS (28,36). In this sense, the mim-pong SG was effective in recovering the patients’ MS, with greater improvements than those obtained with conventional therapy, which involved mobilization, free and resisted active exercises, and stretching. Other research supports these findings (37-39).
Post-stroke muscle dysfunction is a multifactorial phenomenon (40), so there is already evidence that hemiparesis involves factors that go beyond the weakness (40). Thus, therapeutic modalities that provide improvements in MC, in addition to MS, are extremely important. The exercise program using the mim-pong SG is an example of an intervention that has this purpose. In this SG, the score of the game evaluates the MC, where the closer to the center of the racket the patient hits the ball, the higher the score. In this way, the SG provides increased MS using different muscle activation strategies.
After the experimental treatment, there were important improvements in MC only in the patients of the EG. In this group, a significant improvement with a large ES was observed in the QF and HS in the paretic limb (p = 0.000, ES = 0.6/p = 0.000, ES = 1.3) and in the non-paretic limb (p = 0.004, ES = 0.5/p = 0.001, ES = 0.8). The CG only showed significant improvements in the paretic limb, but it was moderate ES (p = 0.003, ES = 0.7/p = 0.006, ES = 0.5). The comparison of these findings is hampered by the fact that there were no studies that analyzed this variable in a similar way.
Although exercises were only performed with the paretic limb, hypotheses can be raised to justify the improvements observed in MS and MC on the contralateral side. A justification for this is related to learning, where the individual presents a greater facility in performing activities in which they already have some experience (11). Another factor that may have resulted in improved MC in the non-paretic limb is the so-called “cross-effect” of training. From the neurological point of view, this can be explained since there are not only intrahemispheric communication pathways but also interhemispheric pathways. The main communication structure between the cerebral hemispheres is the corpus callosum, which consists of the largest set of nerve fibers that perform this function (41), causing the transcortical flow of information and playing an important role in the control of movement (42). Indeed, studies suggest that the integrity of the sensorimotor regions of the corpus callosum correlates with motor function after stroke (43).
In a randomized clinical trial involving 139 patients with stroke, it was found that strength training on the non-hemiparetic side promotes motor function recovery (11). Similarly, a study investigating the effects of non-paretic limb training for improvements in the paretic limb of chronic stroke patients has found that this type of intervention can result in gains related to MS and muscle activation (45). Our research indicated significant improvements with a large ES in MS variable after intervention using the exercise program from the SG in the EG (p = 0.001, ES = 0.6). In the CG, which received treatment based on conventional kinesiotherapy, the improvements were not significant, and the ES was medium (p = 0.247, ES = 0.4). Some studies have used SG, virtual reality, or video games to improve lower limb motor functions in patients with stroke, especially with regard to mobility (46-49). Our findings align with the results of these prior studies. A meta-analysis involving 22 studies found that Wii Fit-based rehabilitation accompanied by conventional therapy results in improvements in functional mobility evaluated with the TUG (46). However, another meta-analysis indicates that there is still a lack of high-quality evidence for the use of virtual reality rehabilitation in stroke treatment (49). It is known that a difference of 2.9 seconds in TUG is the MCID for patients with stroke (50). Thus, in the present study, superiority in the results of the EG in relation to the CG.
Regarding the variable motor impairment, significant improvements were also observed, with large ES in the EG (FMAS p = 0.000, ES = 0.6). Thus, the mim-pong SG can be considered a beneficial resource for motor rehabilitation for patients with stroke. In fact, SG therapy can enhance the effects of conventional rehabilitation when they are used in combination (51).
Patients with stroke commonly face challenges in understanding data indicating the clinical improvements that occur periodically during treatment. In this context, the scores generated by the mim-pong SG can contribute to a clearer perception of the changes observed from one session to another, establishing a more easily comprehensible parameter for comparison. Collectively, the results (MS, MC, FMAS) corroborate with patients’ perceptions as when they were asked about their perception of improvement throughout the clinical trial, some participants in the present study responded that they were getting better because their scores were increasing day by day.
Finally, the present study involved two groups of patients with similar general characteristics: gender, age, body mass index (BMI), laterality, hemiparesis, stroke time, and phase of stroke. This allows a more reliable comparison between the effects of the different treatment proposals used with the groups. It is important to emphasize that most patients from both groups were in the chronic phase, a period characterized by greater difficulty in obtaining improvements when compared to the subacute or acute phase (52). These characteristics of the participants make the results even more valuable since they indicate that the intervention using the mim-pong SG can result in important improvements, even in chronic patients who are often already disillusioned with rehabilitation. Improvements in the chronic phase of stroke are more challenging to achieve compared to the acute or subacute phases. The chronic phase, defined as six months or more after stroke, is characterized by a reduced neuroplastic capacity due to factors such as alterations in cortical activity levels, changes and decreased responsiveness of neuroplastic mechanisms, as well as a reduction in neurotrophic factors such as Brain-Derived Neurotrophic Factor (53,54,55). Thus, since the Serious Game involves specific and high-intensity exercises, it can enhance cortical stimulation, promoting greater neuroplastic activity.
MS training promotes improvements and maintenance of this aspect for up to 4 years post-stroke (50). The present research corroborates with these authors about the existence of improvements in the chronic phase. However, significant improvements were also observed in patients with lesions received approximately eight years ago. This finding may justify the functional improvements that are often achieved with rehabilitation many years after the event (36).
The limitations of our current study include the lack of randomization and a small participant pool, as well as the absence of tools to assess patients’ fatigue and motivation.
Conclusions
In conclusion, our study showed that the exercise program conducted with SG resulted in improvements across all analyzed variables, surpassing the conventional therapy used. Furthermore, correlations were observed between the SG-generated scores and clinical variables, particularly MS and lower limb motor function. Thus, the mim-pong SG can be considered a potential resource for the assessment and treatment of patients with stroke.
For future research, it is recommended to conduct a randomized clinical trial with a larger sample size and to explore the use of the mim-Pong SG with different populations and objectives.
Acknowledgment
The authors would like to thank the institutional support of the University of Joinville Region, the State University of Santa Catarina (UDESC), and Guilherme Guimbala College. The authors would like to thank Alexander Hansen for his editorial assistance.
Disclosures
Conflicts of interest: There is no conflict of interest regarding the present study.
Author contributions: All authors made a significant intellectual contribution to the development of this article, participating in all stages (design, collection, analysis, data interpretation, writing, and reviewing the text). Everyone approved the final version of the article.
References
- 1. Lavis H, Van Vliet P, Tavener M. Stroke survivor, caregiver and therapist experiences of home-based stroke rehabilitation: a thematic synthesis of qualitative studies. Phys Ther Rev. 2023;28(2):157-173. CrossRef
- 2. Campagnini S, Liuzzi P, Mannini A, et al. Effects of control strategies on gait in robot-assisted post-stroke lower limb rehabilitation: a systematic review. J Neuroeng Rehabil. 2022;19(1):52. CrossRef PubMed
- 3. Ahmed T, Islam MR, Brahmi B, et al. Robustness and tracking performance evaluation of PID motion control of 7 DoF anthropomorphic exoskeleton robot assisted upper limb rehabilitation. Sensors (Basel). 2022;22(10):3747. CrossRef PubMed
- 4. Park S, Tang A, Pollock C, et al. Telerehabilitation for lower extremity recovery poststroke: a systematic review and meta-analysis protocol. BMJ Open. 2022;12(3):e055527. CrossRef PubMed
- 5. Xiong F, Liao X, Xiao J, et al. Emerging limb rehabilitation therapy after post-stroke motor recovery. Front Aging Neurosci. 2022;14:863379. CrossRef PubMed
- 6. Wang CY, Olson SL, Protas EJ. Test-retest strength reliability: hand-held dynamometry in community-dwelling elderly fallers. Arch Phys Med Rehabil. 2002;83(6):811-815. CrossRef PubMed
- 7. Eichinger FLF, Soares AV, Noveletto F, et al. Serious game for locomotor rehabilitation of hemiparetic stroke patients. Fisioter Mov. 2020;33:e003316. CrossRef
- 8. Schwarz A, Al-Haj Husain A, Einaudi L, et al. Reliability and validity of a wearable sensing system and online gait analysis report in persons after stroke. Sensors (Basel). 2023;23(2):624. CrossRef PubMed
- 9. Wang YF, Chen WY, Lee CT, et al. Combinations of scalp acupuncture location for the treatment of post-stroke hemiparesis: a systematic review and Apriori algorithm-based association rule analysis. Front Neurosci. 2022;16:956854. CrossRef PubMed
- 10. Demeco A, Zola L, Frizziero A, et al. Immersive virtual reality in post-stroke rehabilitation: a systematic review. Sensors (Basel). 2023;23(3):1712. CrossRef PubMed
- 11. Shao C, Wang Y, Gou H, et al. Strength training of the nonhemiplegic side promotes motor function recovery in patients with stroke: a randomized controlled trial. Arch Phys Med Rehabil. 2023;104(2):188-194. CrossRef PubMed
- 12. Felius RAW, Geerars M, Bruijn SM, et al. Reliability of IMU-based gait assessment in clinical stroke rehabilitation. Sensors (Basel). 2022;22(3):908. CrossRef PubMed
- 13. Winstein CJ, Stein J, Arena R, et al. American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Quality of Care and Outcomes Research. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169. CrossRef PubMed
- 14. Khokale R, S Mathew G, Ahmed S, et al. Virtual and augmented reality in post-stroke rehabilitation: a narrative review. Cureus. 2023;15(4):e37559. CrossRef PubMed
- 15. Phan HL, Le TH, Lim JM, et al. Effectiveness of augmented reality in stroke rehabilitation: a meta-analysis. Appl Sci (Basel). 2022;12(4):1848. CrossRef
- 16. Noveletto F, Soares AV, Mello BA, et al. Biomedical serious game system for balance rehabilitation of hemiparetic stroke patients. IEEE Trans Neural Syst Rehabil Eng. 2018;26(11):2179-2188. CrossRef PubMed
- 17. Mubin O, Alnajjar F, Al Mahmud A, et al. Exploring serious games for stroke rehabilitation: a scoping review. Disabil Rehabil Assist Technol. 2022;17(2):159-165. CrossRef PubMed
- 18. Doumas I, Everard G, Dehem S, et al. Serious games for upper limb rehabilitation after stroke: a meta-analysis. J Neuroeng Rehabil. 2021;18(1):100. CrossRef PubMed
- 19. Noveletto F, Soares AV, Eichinger FLF, et al. Biomedical serious game system for lower limb motor rehabilitation of hemiparetic stroke patients. IEEE Trans Neural Syst Rehabil Eng. 2020;28(6):1481-1487. CrossRef PubMed
- 20. Perrochon A, Borel B, Istrate D, et al. Exercise-based games interventions at home in individuals with a neurological disease: a systematic review and meta-analysis. Ann Phys Rehabil Med. 2019;62(5):366-378. CrossRef PubMed
- 21. Pereira VA, Eldebrando L, Silva HED, et al. Biomedical system to evaluate pulmonary function in patients with post-stroke hemiparesis. Fisioter Mov. 2020;33:e003338. CrossRef
- 22. Fugl-Meyer AR. Post-stroke hemiplegia assessment of physical properties. Scand J Rehabil Med Suppl. 1980;7:85-93. PubMed
- 23. Appelros P. Characteristics of mini-mental state examination 1 year after stroke. Acta Neurol Scand. 2005;112(2):88-92. CrossRef PubMed
- 24. Souza LA, Martins JC, Teixeira-Salmela LF, et al. Validity and reliability of the modified sphygmomanometer test to assess strength of the lower limbs and trunk muscles after stroke. J Rehabil Med. 2014;46(7):620-628. CrossRef PubMed
- 25. Miller W, Jeon S, Ye X. An examination of acute cross-over effects following unilateral low intensity concentric and eccentric exercise. Sports Med Health Sci. 2020;2(3):141-152. CrossRef PubMed
- 26. Cunha BP, Freitas SMSFD, Menezes VVDBD, et al. Ipsilesional upper limb performance in stroke individuals: relationship among outcomes of different tests used to assess hand function. Fisioter Mov. 2016;29(3):561-568. CrossRef
- 27. Billinger SA, Arena R, Bernhardt J, et al. American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Lifestyle and Cardiometabolic Health; Council on Epidemiology and Prevention; Council on Clinical Cardiology. Physical activity and exercise recommendations for stroke survivors: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(8):2532-2553. CrossRef PubMed
- 28. Veldema J, Jansen P. Resistance training in stroke rehabilitation: systematic review and meta-analysis. Clin Rehabil. 2020;34(9):1173-1197. CrossRef PubMed
- 29. Chen SC, Kang JH, Peng CW, et al. Adjustable parameters and the effectiveness of adjunct robot-assisted gait training in individuals with chronic stroke. Int J Environ Res Public Health. 2022;19(13):8186. CrossRef PubMed
- 30. Lodha N, Patel P, Casamento-Moran A, et al. Strength or motor control: what matters in high-functioning stroke? Front Neurol. 2019;9:1160. CrossRef PubMed
- 31. Verrienti G, Raccagni C, Lombardozzi G, et al. Motivation as a measurable outcome in stroke rehabilitation: a systematic review of the literature. Int J Environ Res Public Health. 2023;20(5):4187. CrossRef PubMed
- 32. Dorsch S, Ada L, Sorial T, et al. The relationship between strength of the affected leg and walking speed after stroke varies according to the level of walking disability: a systematic review. Phys Ther. 2021;101(12):pzab233. CrossRef PubMed
- 33. Harjpal P, Qureshi MI, Kovela RK, et al. Efficacy of bilateral lower-limb training over unilateral lower-limb training to reeducate balance and walking in post-stroke survivors: a randomized clinical trial. Cureus. 2022;14(10):e30748. CrossRef PubMed
- 34. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. 1989;10(4):407-415. CrossRef PubMed
- 35. Lee MY, Sung KS, Ham H, et al. Knee extensor strength measurement in patients with limited physical activity using a supine dynamometer anchoring frame. Ann Rehabil Med. 2020;44(6):502-509. CrossRef PubMed
- 36. Veerbeek JM, van Wegen E, van Peppen R, et al. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLoS One. 2014;9(2):e87987. CrossRef PubMed
- 37. Viana RB, de Oliveira VN, Dankel SJ, et al. The effects of exergames on muscle strength: a systematic review and meta-analysis. Scand J Med Sci Sports. 2021;31(8):1592-1611. CrossRef PubMed
- 38. Park JS, Lee G, Choi JB, et al. Game-based hand resistance exercise versus traditional manual hand exercises for improving hand strength, motor function, and compliance in stroke patients: a multi-center randomized controlled study. NeuroRehabilitation. 2019;45(2):221-227. CrossRef PubMed
- 39. Tăut D, Pintea S, Roovers JWR, et al. Play seriously: effectiveness of serious games and their features in motor rehabilitation. A meta-analysis. NeuroRehabilitation. 2017;41(1):105-118. CrossRef PubMed
- 40. Hunnicutt JL, Gregory CM. Skeletal muscle changes following stroke: a systematic review and comparison to healthy individuals. Top Stroke Rehabil. 2017;24(6):463-471. CrossRef PubMed
- 41. Chang SH, Francisco GE, Zhou P, et al. Spasticity, weakness, force variability, and sustained spontaneous motor unit discharges of resting spastic-paretic biceps brachii muscles in chronic stroke. Muscle Nerve. 2013;48(1):85-92. CrossRef PubMed
- 42. Ocklenburg S, Gerding WM, Arning L, et al. Myelin genes and the corpus callosum: proteolipid protein 1 (PLP1) and contactin 1 (CNTN1) gene variation modulates interhemispheric integration. Mol Neurobiol. 2017;54(10):7908-7916. CrossRef PubMed
- 43. Stewart JC, Dewanjee P, Tran G, et al. Role of corpus callosum integrity in arm function differs based on motor severity after stroke. Neuroimage Clin. 2017;14:641-647. CrossRef PubMed
- 44. Li Y, Wu P, Liang F, et al. The microstructural status of the corpus callosum is associated with the degree of motor function and neurological deficit in stroke patients. PLoS One. 2015;10(4):e0122615. CrossRef PubMed
- 45. Dragert K, Zehr EP. High-intensity unilateral dorsiflexor resistance training results in bilateral neuromuscular plasticity after stroke. Exp Brain Res. 2013;225(1):93-104. CrossRef PubMed
- 46. Ghazavi Dozin SM, Mohammad Rahimi N, Aminzadeh R. Wii fit-based biofeedback rehabilitation among post-stroke patients: a systematic review and meta-analysis of randomized controlled trial. Biol Res Nurs. 2024;26(1):5-20. CrossRef PubMed
- 47. Spina S, Facciorusso S, D’Ascanio MC, et al. Sensor based assessment of turning during instrumented Timed Up and Go Test for quantifying mobility in chronic stroke patients. Eur J Phys Rehabil Med. 2023;59(1):6-13. CrossRef PubMed
- 48. Lenkulkul F, Franco G, Soares AV, et al. Jogo Sério para reabilitação de hemiparéticos por acidente vascular cerebral: impacto na qualidade de vida. RSD. 2022;11(14):e87111435976. CrossRef
- 49. Peng QC, Yin L, Cao Y. Effectiveness of virtual reality in the rehabilitation of motor function of patients with subacute stroke: a meta-analysis. Front Neurol. 2021;12:639535. CrossRef PubMed
- 50. Flansbjer UB, Holmbäck AM, Downham D, et al. Reliability of gait performance tests in men and women with hemiparesis after stroke. J Rehabil Med. 2005;37(2):75-82. CrossRef PubMed
- 51. Soares AV, Borges Júnior NG, Hounsell MS, et al. A serious game developed for physical rehabilitation of frail elderly. European Research in Telemedicine/La Recherche Européenne En Télémédecine. 2016;5:45-53. CrossRef
- 52. Van Hoornweder S, Vanderzande L, Bloemers E, et al. The effects of transcranial direct current stimulation on upper-limb function post-stroke: a meta-analysis of multiple-session studies. Clin Neurophysiol. 2021;132(8):1897-1918. CrossRef PubMed
- 53. Dromerick AW, Geed S, Barth J, et al. Critical Period After Stroke Study (CPASS): a phase II clinical trial testing an optimal time for motor recovery after stroke in humans. Proc Natl Acad Sci USA. 2021;118(39):e2026676118. CrossRef PubMed
- 54. Mojtabavi H, Shaka Z, Momtazmanesh S, et al. Circulating brain-derived neurotrophic factor as a potential biomarker in stroke: a systematic review and meta-analysis. J Transl Med. 2022;20(1):126. CrossRef PubMed
- 55. Murphy TH, Corbett D. Plasticity during stroke recovery: from synapse to behaviour. Nat Rev Neurosci. 2009;10(12):861-872. CrossRef PubMed