|
Arch Physioter 2024; 14: 182-188 ISSN 2057-0082 | DOI: 10.33393/aop.2024.3155 ORIGINAL RESEARCH ARTICLE |
Evolving trends of systematic reviews on virtual reality for stroke rehabilitation
Silvia Bargeri1, Mariachiara Baggio2, Stefania Guida![]() 1, Greta Castellini1, Silvia Gianola
1, Greta Castellini1, Silvia Gianola![]() 1
1
ABSTRACT
Objective: Virtual reality (VR) therapies have increasingly been adopted across medical fields, including neurorehabilitation for stroke recovery. Evidence from several systematic reviews (SRs) was explored, covering different aspects. We aim to explore overlaps, gaps, and trends of SRs focusing on VR stroke rehabilitation providing a foundation for improving the field and addressing current limitations.
Materials and methods: We moved from a recent overview of reviews, searching multiple databases for all published SRs and the international database of prospectively registered SRs (PROSPERO) for ongoing SRs. Data extraction of study characteristics and methodological quality of SRs using AMSTAR 2 were obtained from a recent overview of reviews. Two independent reviewers conducted data analysis and visualization by the trend over time of published SRs with their included primary studies and ongoing SRs, methodological quality and other SR characteristics.
Results: The data set consisted of 58 SRs, including 345 primary studies and 45 ongoing SRs, published between 2007 and 2022. The number of published and ongoing SRs significantly increased over time (R2 = 0.8654; R2 = 0.747, respectively). In the last three years, Asia accounts for the majority of publications (31%). Overall, the main outcome assessed over time was upper extremity function and activity in 67.2% of SRs. Most of the published SRs were judged “critically low” (77.6%). The number of included studies increased over time reaching a median of 17 studies with a median of 493 participants.
Conclusions: In stroke rehabilitation, the published and ongoing SRs on VR have risen over time in terms of the number of publications, with some concerns about methodological quality and representation of countries around the world.
Keywords: Randomized controlled trials as topic, Rehabilitation, Stroke, Systematic review, Virtual reality
Received: June 4, 2024
Accepted: December 5, 2024
Published online: December 31, 2024
This article includes supplementary materials
Corresponding author:
Stefania Guida
email: stefania.guida@grupposandonato.it
Archives of Physiotherapy - ISSN 2057-0082 - www.archivesofphysiotherapy.com
© 2024 The Authors. This article is published by AboutScience and licensed under Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0).
Commercial use is not permitted and is subject to Publisher’s permissions. Full information is available at www.aboutscience.eu
What is already known about this topic:
- In recent years, VR technologies rapidly spread across medical specialties, including neurorehabilitation. Recent research trends highlight various VR therapies, but systematic reviews (SR) on VR for stroke rehabilitation, crucial for clinicians and policymakers, remain unexplored.
What does the study add:
- The number of SRs on VR has increased, including those ongoing, with larger sample sizes and diverse outcomes. However, concerns about methodological quality and global representation exist. Authors should check protocol registries and plan innovative synthesis methods.
INTRODUCTION
Stroke is one of the major causes of disability and death worldwide, with the highest incidence in the elderly population (1). In 2019, ischemic heart disease and stroke were the top-ranked causes of Disability-Adjusted Life-Years (DALYs) both in the 50–74-year-old group and in the 75-year-old and elder group (2,3), impacting motor functions, activities of daily living (ADL), social participation and quality of life (4).
The use of technology in rehabilitation after stroke has been proposed worldwide in the past three decades, with an increasing interest in virtual reality (VR) (5). VR technology has the advantages of creating more realistic environments to imitate the real world, providing repetitive training for specific tasks, increasing the sense of participation, and stimulating near-life experiences that patients cannot otherwise achieve (6). In fact, VR rehabilitation utilizes virtual environments and objects to deliver visual and auditory feedback to the user. This feedback can be experienced through various platforms, such as head-mounted displays, projection systems, or flat screens, with equipment ranging from basic tools like a joystick to technologies such as sensors or cameras. The implementation of VR in rehabilitation shows helpful results in motor function recovery, especially in the upper extremities and lower extremities for balance, gait, and posture. The way that VR can be used in multiple different conditions suggests the efficacy and versatility of the application (6).
In recent years, especially during the pandemic, there has been a rapid spread of VR technologies (7,8) across all medical specialties (9), including the neurorehabilitation field (10). The most recent research trends cover more defined types of VR therapy, embracing different study designs offering information regarding the current hotspots in the field (10). However, to our knowledge, the characteristics, and extent of the highest study design for synthesizing the evidence (i.e., SRs) and informing clinicians, patients, and policymakers focused on stroke VR rehabilitation was not investigated yet. Therefore, we aimed to evaluate overlaps, gaps, and trends of published and ongoing SRs on VR for stroke rehabilitation over the years, along with their general characteristics and methodological quality.
METHODS
Study design
We conducted a cross-sectional study based on an overview of reviews (11). We adapted items from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) (12), assuming as units of analysis the included SRs (see Supplementary 1).
Search strategy and data collection
We moved from a recent overview of reviews (11) investigating VR on stroke (CRD42022329263), which included 58 SRs and 345 unique primary studies.
The search was launched in multiple databases (the Cochrane Database of Systematic Reviews, EMBASE, MEDLINE, Scopus, ISI Web of Science, CINAHL, PsycINFO, PEDro, Otseeker, Healthevidence.org, Epistemonikos), including PROSPERO for ongoing SRs from inception up to January 17, 2023. We selected SRs published in English including adults with any diagnosis of stroke. The treatment investigated was any kind of immersive, semi-immersive, or non-immersive VR intervention, either with or without conventional therapy (e.g., usual care, exercises). Details of eligibility criteria are reported in our previous publication (11).
Data collection
We obtain the dataset of the related overview (11) to collect information about the general characteristics and methodological quality of SRs. Particularly, we used the following general characteristics: years of publication, countries of the corresponding author, description of outcomes, references and year of included primary studies, number of included primary studies, sample size, journal of publication, and journal impact factor (JIF), methodological quality appraised by A Measurement Tool to Assess SR (AMSTAR) 2 and categorized into critically low, low, moderate, and high methodological quality (13).
Data synthesis
We used descriptive statistics for general characteristics and methodological quality expressed as median and interquartile range (IQR) or absolute value and frequency.
The data chart and Pearson’s correlation coefficient were used to assume linearity assumption. Data were transformed into a logarithmic scale. Prediction of the percentage of published and ongoing SR data based on year was computed through linear regression models plotted with confidence and prediction intervals at 95%. All analyses were performed using the R Core Team (2023) (14).
We then visually described the trend of the following variables: median JIF, number of included primary studies and participants, outcomes, and methodological quality using Microsoft Excel 2019 and RAWGraphs 2.0 (15).
RESULTS
Publication trend
Overall, the data set consisted of 58 SRs published between 2007 and 2022, including 345 primary studies published between 1999 and 2021, and 45 ongoing SRs from 2014 to 2022. We found a significant increase in the number of published and ongoing SRs over the years (R2 = 0.8654; R2 = 0.747) respectively) (Figure 1). In Supplementary 2, we reported the trend of SRs and primary studies publication for each year (Figure S1-S2, respectively).
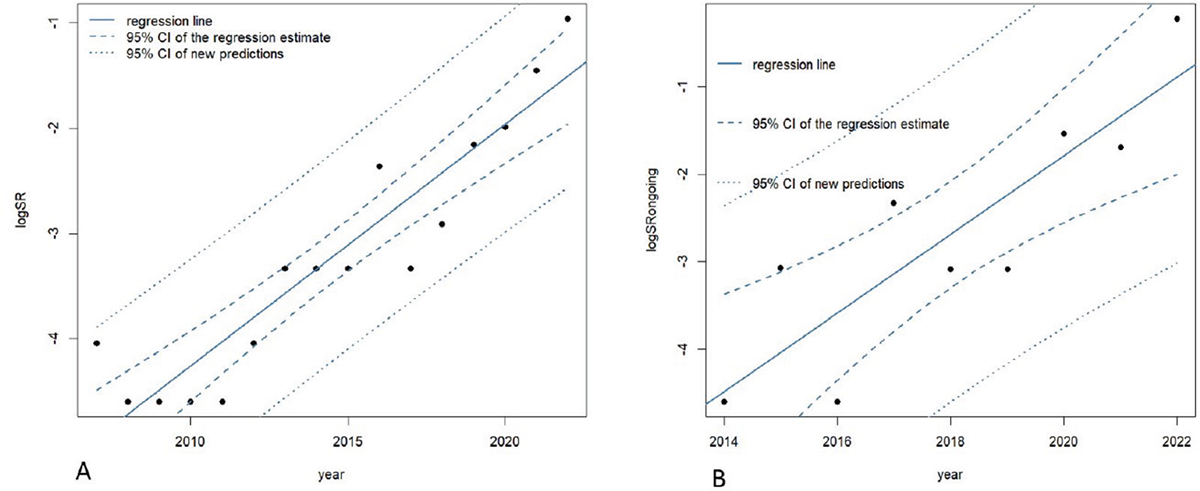
FIGURE 1 - A) Trend of published SR and B) Trend of ongoing SR over the years. Legend: SRs, systematic reviews.
General characteristics of published systematic reviews
In Table 1 we showed overall general characteristics of published SRs. Most SRs include RCTs only (81%). Overall, 42 SRs (72.4%) conducted meta-analyses. Many SRs (69%) included mixed onset of stroke. The most common journal of publication was the Journal of Stroke and Cerebrovascular Diseases (8.6%) (Supplementary 2, Table S1). The median JIF was 3.25 (2.18-4.61). The distribution of the median JIF over the years is reported in Supplementary 2, Figure S3.
| General Characteristics | Overall (N = 58) |
|---|---|
| Population, Median (IQR) | 492.5 (224.8-1082.8) |
| N. of included primary studies, median (IQR) | 17 (8-30.3) |
| N of outcomes, median (IQR) | 3 (2-4) |
| Presence of conflicts of interest, N (%) | 6 (10.3) |
| Non-industry funding, N (%) | 28 (48.3) |
| Presence of meta-analyses, N (%) | 42 (72.4) |
| SR including RCTs only, N (%) | 47 (81.0) |
| Country, n (%) | |
| Africa | 1 (1.7) |
| America | 13 (22.4) |
| Asia | 24 (41.4) |
| Europe | 16 (27.6) |
| Oceania | 4 (6.9) |
| JIF, Median (IQR) | 3.25 (2.18-4.61) |
| Outcomes, N (%) | Total (n = 58) |
| Upper limb function and activity | 39 (67.2) |
| Gait and balance | 36 (62.1) |
| ADL | 37 (63.8) |
| Participation | 28 (48.3) |
| Cognitive and mental function | 20 (34.5) |
| Adverse events | 18 (31.0) |
Primary studies and participants of included SRs
The number of primary studies included in an SR ranged from a minimum of three to a maximum of 87, with a median of 17 per SR. More than 85% of primary studies were RCTs. The number of participants included in the SRs ranged from a minimum of 60 to a maximum of 3540, with a median of 493. Supplementary 2, Figure S4-S5 shows the distribution of primary studies and participants over the years.
Countries
As regards the Asian states, China is the first country for the number of reviews, with 15 publications (25.9% of all SRs). In Europe, 16 SRs were published in eight different countries; Spain holds 5 publications (8.6% of all SRs), whereas Italy and Belgium hold 3 reviews each one (5.2%). America is the third continent for publications of SRs, with Brazil involved in 6 studies (10.3%), Canada in 4 (6.9%), and the USA in 3 (5.2%). In Oceania, 4 SRs were published. Only one review was conducted in Africa. The distribution of the continents where SRs have been conducted both generally and over the years is illustrated in Figure 2A-B. In the last three years we found an absolute increase in publications in Asia (n = 18, 31% of the overall sample).
Outcomes
Overall, the main outcome assessed was Upper Extremity Function and Activity in 67.2% of SRs (n = 39), followed by Activities of Daily Living (n = 37) and Gait and Balance (n = 36). Less investigated outcomes were Participation (n = 28), Cognitive and Mental function (n = 20), and Adverse Events (n = 18) (Table 1). Figure 3 shows the outcome distribution over the years. In the last three years, 28 SRs (48.3% of the overall sample) assessed Upper Limb Function and Activity.
Methodological quality
According to the AMSTAR 2 tool, 45 SRs (77.6%) were judged critically low, 12 low (20.7%), and one high (1.7%). Overall, 69% of SRs have no recorded protocol, and 89.7% do not describe motivations for the excluded primary studies. The 96.6% of SRs accomplished exhaustive bibliographic research. As regards the quality of the primary studies included in the 58 SRs, all authors used an adequate tool to measure the risk of bias (100%), and 74.1% included the assessment of primary studies in their SRs’ results (Supplementary File 2, Figure S6). Figure 4 shows the methodological quality distribution over the years.
DISCUSSION
Main findings
We analyzed the frequency and characteristics of 58 published SRs and 45 ongoing SRs covering the scientific diffusion of VR technologies for stroke from 2007 to 2022 and from 2014 to 2022, respectively, with an increasing trend over the years.
VR research is becoming more influential around the world, with over one-fifth of all countries involved in the scientific progress in this field (16). Asia represents the most influential country regarding VR rehabilitation in stroke adult people, with a particular increase in SR’s publications in the last three years (31%). In particular, China has been the leader in SR publications since it started in 2007 to cover not only the VR scientific field but also all medical fields, as it is in the top publishing countries, as reported by recent publications (17,18). With its aging population, China faces increasing challenges for stroke care and prevention, with a prevalence of stroke survivors of 58.1 million, four times higher than other countries (19). It has been argued that this rapid increase in the number of SRs could be due to multiple reasons, including the easiest widely accessible tools for doing SRs and meta-analyses (20), the pressures of academia (21), or industry of contracting companies “operating in the domain of evidence synthesis” to produce these publications, many of which probably remain unpublished (22). However, we cannot exclude that this increase is due to the growth of collaborative research with China and other countries, as already reported (23)
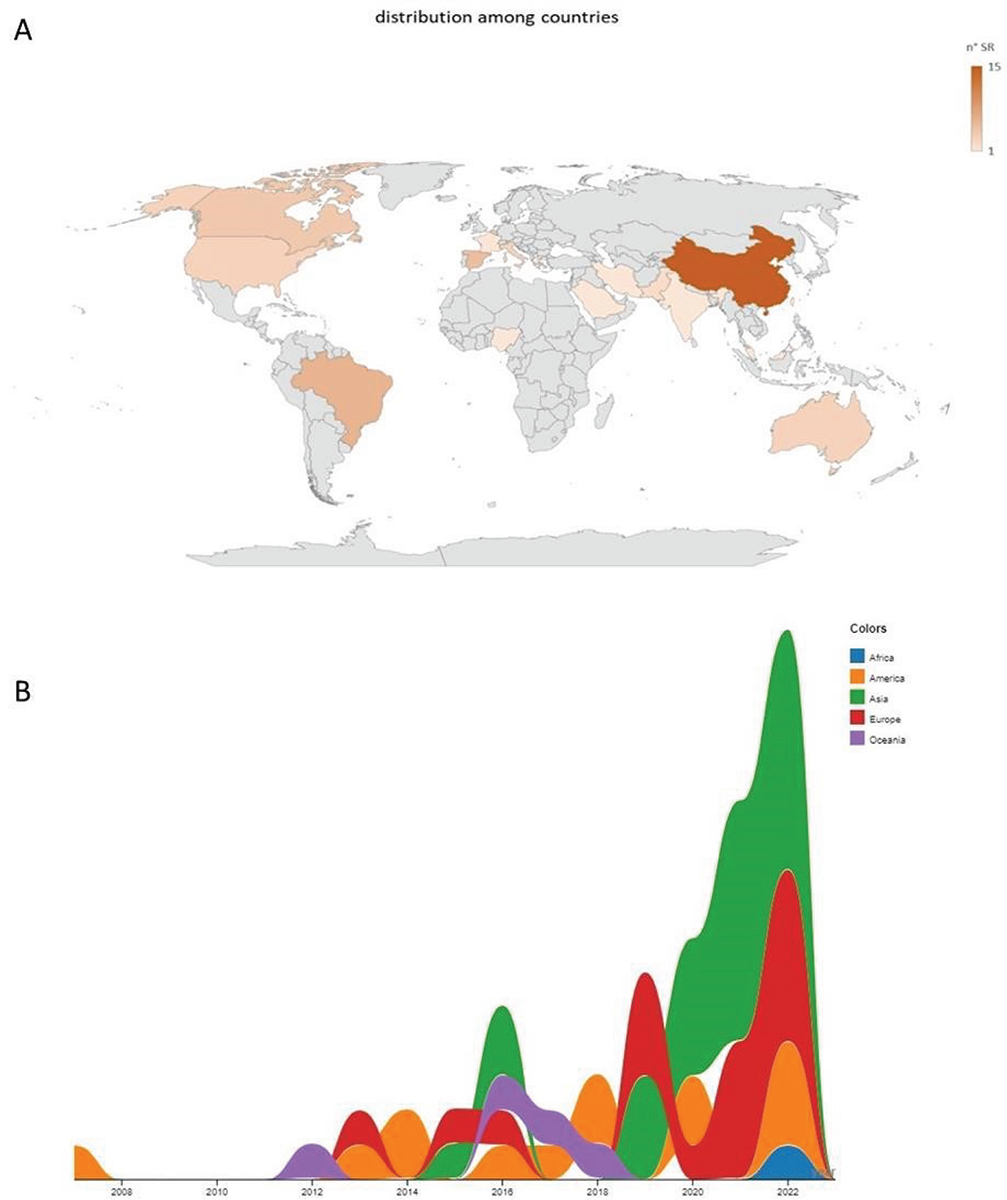
FIGURE 2 - Countries of corresponding authors of SRs A) overall and B) over the years. Legend: the size is proportional to the number of SRs for each year by country
As the number of SRs has increased over time, the number of participants included in SRs and the number of included primary studies increased. This phenomenon might be conditioned by the fact that the latest published SRs can also include primary studies as well as participants of the oldest SRs. However, the number of primary studies retrieved from SRs may be underestimated considering that a time span exists from running the search strategy and publication of SRs (24); therefore, we cannot exclude that some published primary studies were not included in the SRs as well as new primary studies might be actually still ongoing. The year 2019-2020 was represented by a global pandemic emergency with limited possibilities to undergo primary studies. This might explain the substantial growth of secondary literature studies rather than primary studies in the last recent years.
Looking at the health outcomes, upper limb function and activity, participation, and cognitive and mental function are becoming more assessed in SRs as a sign of implementation of a core outcome set that can optimize the quality of poststroke rehabilitation (24).
We also found that the methodological quality of SRs remained critically low over time, even if SRs were published in journals with a median JIF of 3.25. It has been found that JIF may have little to no association with study results or methodological quality (25). Low methodological quality can be mainly due to some critical flaws in the protocol and in the excluded studied justification items. In fact, according to AMSTAR 2, 69% of our included SRs have no explicit statement that the study methods were established prior to the conduct of the review. On one hand, these findings are discouraging, as more than half of the authors (55.8%) register their protocol prior to publishing their systematic review/meta-analysis (26). Pre-registration does not guarantee that the protocol is complete but allows readers to be aware of methods for conducting and reporting in a transparent way (22). On the other hand, in the last years, we collected many ongoing SRs pre-registered in PROSPERO as a starting point of improvement for this flaw. However, authors should use registers such as PROSPERO to check overlapping questions covered by already existing SRs to avoid redundant meta-analyses with inconsistency and discordant findings. As well, journal editors should keep in mind that much has already been published. Multiple overlapping SRs can facilitate the origin of disputes. This is well known also in other fields such as the case of thrombolytic therapy for pulmonary embolism (27). As well, the large increase in the number of published and ongoing SRs over the years raises concerns about research waste. It should be ethical and reasonable to systematically review what is already known before deciding to perform any new study (28).
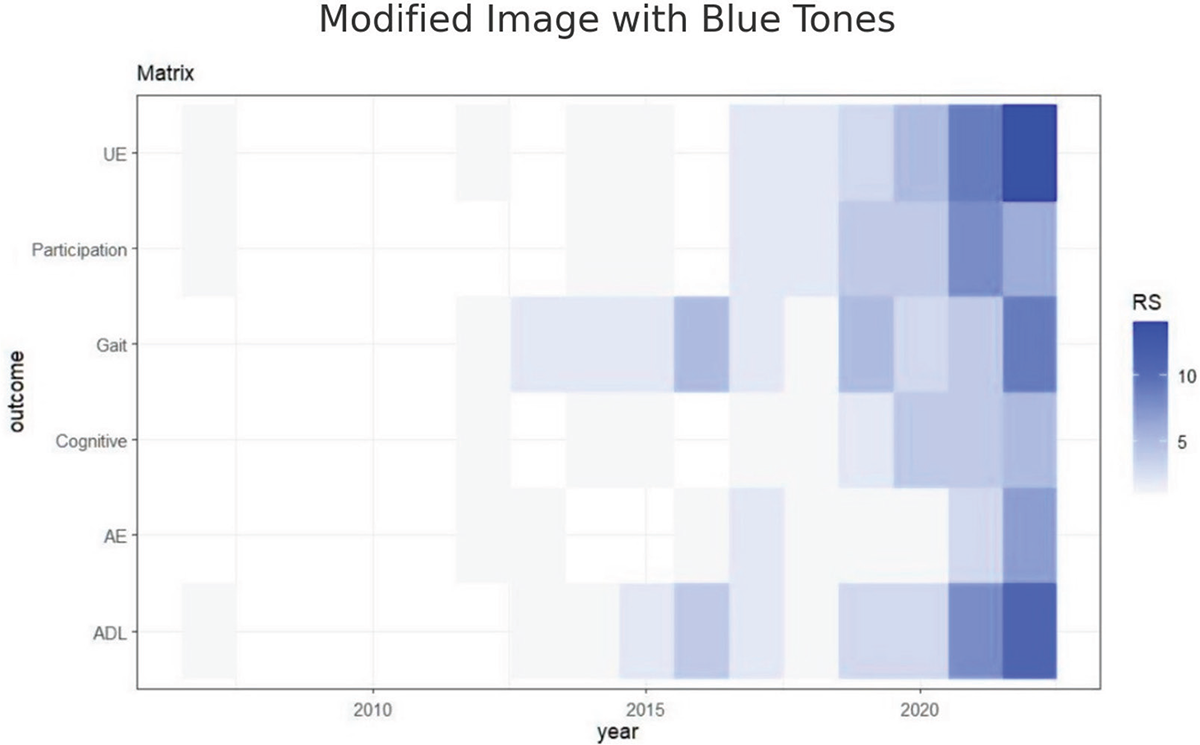
FIGURE 3 - Outcome assessed in SRs over years. Legend: AE, adverse events, UE, upper limb
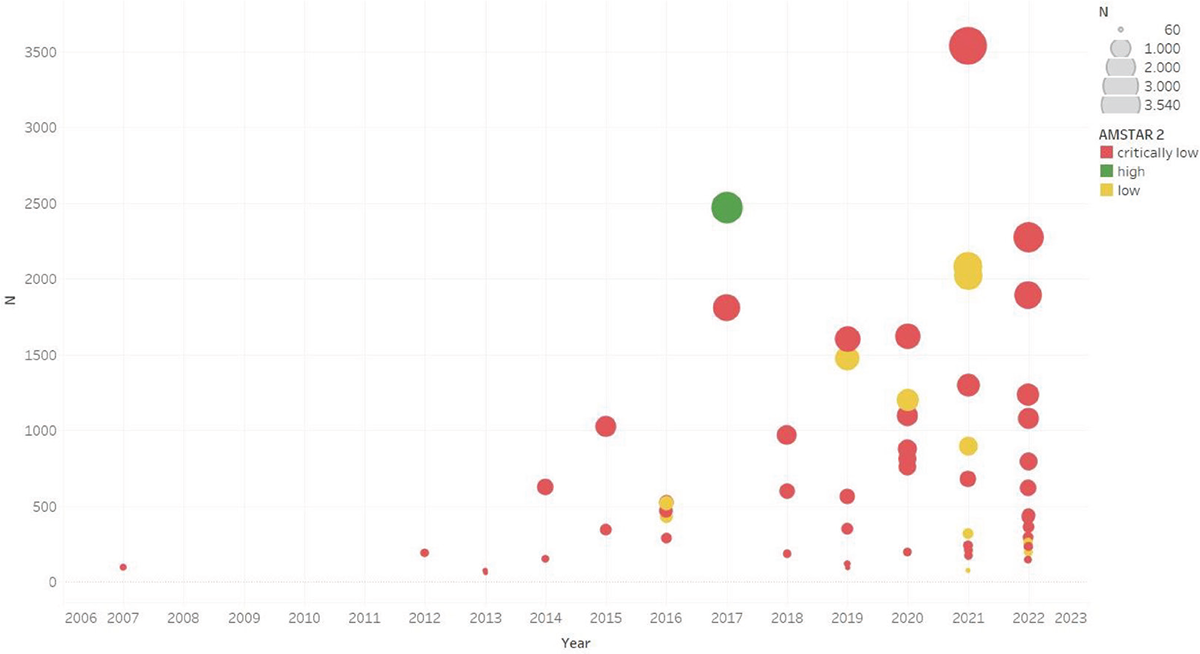
FIGURE 4 - Methodological quality of SRs over the years. Legend: the bubble size is proportional to the number of included participants in each SR
The other important flaw in SRs is related to the non-reporting of studies excluded from SRs. We found the 89.7% don’t provide a list of the excluded studies and the motivation. This can lead to selective inclusion for outcome non-reporting bias impacting meta-analytic effects (2930-31).
Recently, a meta-epidemiological study found that 58,8% of the included SRs (n = 131) excluded studies due to “no relevant outcome data” (32) despite it not being recommended by the scientific community (33) since this may be a consequence of selective outcome reporting and therefore compromise the systematic review reliability.
Strength and limitation
This review aimed to summarize all the publications and trends about the application of VR in the neurorehabilitation field in adult people with stroke. To analyze this specific sample, we included a total of 103 papers (58 published and 45 ongoing SRs) without limits in a publication year. An exhaustive research was conducted in many different databases. This trend study is linked to an extensive overview of reviews in accordance with the Cochrane Guidelines; moreover, the review protocol was registered in the PROSPERO database.
Limitations of this work need to be acknowledged. The research was conducted for only English-language publications, and the children population was excluded from the sample. We did not extract data from primary studies focused on VR rehabilitation, but we reported the trend of publications of those included in the SRs. Ongoing SRs were searched on PROSPERO and not on other registries. Nevertheless, PROSPERO seems to be the most common database used for protocol registration [71.3%, n = 270 (26)]. Thus, we cannot be sure that all SRs included the whole body of evidence.
Conclusion
The highest synthesis of evidence as published SRs, including those ongoing on VR, has risen over time in terms of the number of publications, sample size, and eligible outcomes, with some concerns about methodological quality and representation of countries around the world. To avoid waste of research, authors should check protocol registries before embarking on a new systematic review. As well they should consider planning innovative research methods for synthetizing the amount of literature available.
Disclosures
Conflict of interest: The authors declare no conflict of interest
Financial support: This study was supported and funded by the Italian Ministry of Health. The APC was funded by the Italian Ministry of Health – Ricerca Corrente. The funder had no role in study design, data collection and analysis, decision to publish, or manuscript preparation.
Author’s contributor role: SB: conceptualization, data curation, data analysis, writing the original draft, reviewing and editing; MB: data curation, data analysis, writing the original draft, reviewing and editing; SG: data analysis, writing the original draft, reviewing & editing; GC: methodology, writing the original draft, reviewing & editing; SG: conceptualization, methodology, reviewing and editing;
Data Availability Statement: Data publicly available: The data presented in this study are openly available in the OSF online repository at https://osf.io/v6k75/
References
- 1. Sacco RL, Kasner SE, Broderick JP, et al. American Heart Association Stroke Council, Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; Council on Peripheral Vascular Disease; Council on Nutrition, Physical Activity and Metabolism. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064-2089. CrossRef PubMed
- 2. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204-1222. CrossRef PubMed.
- 3. Katan M, Luft A. Global Burden of Stroke. Semin Neurol. 2018;38(2):208-211. CrossRef PubMed
- 4. Hatem SM, Saussez G, Della Faille M, et al. Rehabilitation of motor function after stroke: A multiple systematic review focused on techniques to stimulate upper extremity recovery. Front Hum Neurosci. 2016;10:442. CrossRef PubMed
- 5. Laffont I, Van Dokkum L, Froger J, et al. Stroke patients: emerging rehabilitation techniques. Ann Phys Rehabil Med. 2012;55:e145-e146. CrossRef
- 6. Amirthalingam J, Paidi G, Alshowaikh K, et al. Virtual reality intervention to help improve motor function in patients undergoing rehabilitation for cerebral palsy, Parkinson’s disease, or stroke: A systematic review of randomized controlled trials. Cureus. 2021;13(7):e16763. CrossRef PubMed
- 7. Ahmadi Marzaleh M, Peyravi M, Azhdari N, et al. Virtual reality applications for rehabilitation of COVID-19 patients: A systematic review. Health Sci Rep. 2022;5(6):e853. CrossRef PubMed
- 8. Pallavicini F, Pepe A, Clerici M, et al. Virtual reality applications in medicine during the COVID-19 pandemic: Systematic review. JMIR Serious Games. 2022;10(4):e35000. CrossRef PubMed
- 9. Kacmaz KS, Kaçmaz C. Bibliometric analysis of research in pediatrics related to virtual and augmented reality: A systematic review. Curr Pediatr Rev. 2024;20(2):178-187. CrossRef PubMed
- 10. Guo QF, He L, Su W, et al. Virtual reality for neurorehabilitation: A bibliometric analysis of knowledge structure and theme trends. Front Public Health. 2022;10:1042618. CrossRef. PubMed
- 11. Bargeri S, Scalea S, Agosta F, et al. Effectiveness and safety of virtual reality rehabilitation after stroke: an overview of systematic reviews. EClinicalMedicine. 2023;64:102220. CrossRef PubMed
- 12. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573-577. CrossRef PubMed
- 13. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. CrossRef PubMed
- 14. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Online (Accessed June 2024)
- 15. Mauri M, Elli T, Caviglia G, et al. RAWGraphs: A visualisation platform to create open outputs. In Proceedings of the 12th Biannual Conference on Italian SIGCHI Chapter, 2017; 28: 1-5. CrossRef
- 16. Pawassar CM, Tiberius V. Virtual reality in health care: Bibliometric analysis. JMIR Serious Games. 2021;9(4):e32721. CrossRef PubMed
- 17. Fontelo P, Liu F. A review of recent publication trends from top publishing countries. Syst Rev. 2018;7(1):147. CrossRef PubMed
- 18. Hoffmann F, Allers K, Rombey T, et al. Nearly 80 systematic reviews were published each day: Observational study on trends in epidemiology and reporting over the years 2000-2019. J Clin Epidemiol. 2021;138:1-11. CrossRef PubMed
- 19. World stroke organization (WSO). Global Stroke Fact Sheet 2022. Extracted from Global Burden of Disease Stroke Statistics Worldwide for the year 2019. Online (Accessed June 2024)
- 20. Ye XF, Yu DH, He J. The rise in meta-analyses from China. Epidemiology. 2013;24(2):335-336. CrossRef PubMed
- 21. Yang ZP, Ye XF, Fan DM. Meta-analysis is victim to Chinese academic and educational systems. J Formos Med Assoc. 2013 May;112(5):235-6. CrossRef PubMed
- 22. Ioannidis JP. The mass production of redundant, misleading, and conflicted systematic reviews and meta-analyses. Milbank Q. 2016;94(3):485-514. CrossRef PubMed
- 23. Wagner CS, Park HW, Leydesdorff L. The continuing growth of global cooperation networks in research: A conundrum for national governments. PLoS One. 2015;10(7):e0131816. CrossRef PubMed
- 24. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. CrossRef PubMed
- 25. Saginur M, Fergusson D, Zhang T, et al. Journal impact factor, trial effect size, and methodological quality appear scantly related: a systematic review and meta-analysis. Syst Rev. 2020;9(1):53. CrossRef PubMed
- 26. Tawfik GM, Giang HTN, Ghozy S, et al. Protocol registration issues of systematic review and meta-analysis studies: a survey of global researchers. BMC Med Res Methodol. 2020;20(1):213. CrossRef PubMed
- 27. Riva N, Puljak L, Moja L, et al. Multiple overlapping systematic reviews facilitate the origin of disputes: the case of thrombolytic therapy for pulmonary embolism. J Clin Epidemiol. 2018;97:1-13. CrossRef PubMed
- 28. Clarke M, Alderson P, Chalmers I. Discussion sections in reports of controlled trials published in general medical journals. JAMA. 2002;287(21):2799-2801. CrossRef PubMed
- 29. Page MJ, Forbes A, Chau M, et al. Investigation of bias in meta-analyses due to selective inclusion of trial effect estimates: empirical study. BMJ Open. 2016;6(4):e011863. CrossRef PubMed
- 30. Kirkham JJ, Altman DG, Williamson PR. Bias due to changes in specified outcomes during the systematic review process. PLoS One. 2010;5(3):e9810. CrossRef PubMed
- 31. Page MJ, McKenzie JE, Kirkham J, et al. Bias due to selective inclusion and reporting of outcomes and analyses in systematic reviews of randomised trials of healthcare interventions. Cochrane Database Syst Rev. 2014;2014(10):MR000035. CrossRef PubMed
- 32. Lazzarini SG, Stella Yousif M, Bargeri S, et al. Reasons for missing evidence in rehabilitation meta-analyses: a cross-sectional meta-research study. BMC Med Res Methodol. 2023;23(1):245. CrossRef PubMed
- 33. Higgins JPT, Lasserson T, Chandler J, et al. Methodological Expectations of Cochrane Intervention Reviews. Cochrane: London, Version February 2022. Online