|
AboutOpen | 2020; 7(1): 80-88
ORIGINAL RESEARCH ARTICLE |
Socioeconomic impact of migraine in Italy: Results of a national survey
Abstract
Background: Literature data indicate that migraine has a stronger impact on both healthcare consumption and quality of life (QoL) in women.
Objectives: The objective of this article is to evaluate out-of-pocket (OoP) costs, productivity losses and cost of informal care of migraine in Italy, with a special focus on the detection of potential differences between male and female subjects.
Methods: A cross-sectional study was conducted. Data were collected via a web-based survey platform, which included a socioeconomic questionnaire (five sections: clinical history; occupational status; informal assistance; visits, exams and treatments; and loss of productivity) and two questionnaires on QoL (EuroQol 5D 5L and Migraine-Specific Questionnaire, MSQ).
Results: Six hundred and seven participants took part in the survey (average age of 42 years; female 70%). The duration of the attack (4-72 hours) was significantly much longer in women than in men (71% vs. 49%; p < 0.001). Seventy per cent of the sample reported to be employed. Lower income was associated with women (p < 0.001). Men received more informal assistance days than women (5.2 vs. 3.9 days; p = 0.007). The quarterly cost including OoP costs, informal assistance and lost productivity averaged €1,088 and was higher for men compared to women (€1,515 vs. €908; p < 0.001). The MSQ reported a significantly worse QoL for women.
Conclusion: The results seemed to prove that migraine is a gender disease. Moreover, a potentially unequal access to informal assistance and healthcare resources not covered by the Italian National Health Service is highlighted for women because of their lower average income and purchasing power compared to men.
Keywords: Cost, Gender difference, Migraine, Out-of-pocket costs, Productivity losses, Quality of life
Received: September 22, 2020
Accepted: October 21, 2020
Published online: December 10, 2020
© 2020 The Authors. This article is published by AboutScience and licensed under Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC-ND 4.0). Any commercial use is not permitted and is subject to Publisher’s permissions. Full information is available at www.aboutscience.eu
Background
Migraine is a neurological disabling disease characterized by recurrent headache attacks lasting from 4 to 72 hours (1).
Based on the number of days of headache, migraine is classified as episodic or chronic, with the latter reaching a prevalence rate of 0.28% (2). Migraine is defined as chronic if headache is present on at least 15 days per month and for a minimum of 3 months, during which there must be headache for at least 8 days per month to meet the diagnostic criteria of migraine (3); it is defined as episodic if headache is present on less than 15 days per month (4).
Migraine is one of the main causes of disability (5), especially across the most productive population age group (15-49 years) (6). Severe disability due to migraine is a major cause of reduction in quality of life (QoL), diminished productivity and increased utilization of healthcare resources, translating into higher costs for both the individual and society (7-9). In Europe, migraine is considered as one among the costliest neurological diseases (8, 10).
According to a literature review, the average annual cost for managing an individual with migraine varies from €1,222 (11) to €11,400 (12), depending on the perspective chosen and the costs considered. Although the evidence is limited, the consumption of healthcare services (drugs, complementary medicine, clinical visits) is higher among women than men (13-16). Loss of productivity is similar between genders, with higher costs for chronic migraine (CM) (17). Generally, according to literature, a higher number of paid lost working days is reported for men, while a higher number of unpaid (housework) lost working days is reported for women (17-20). Finally, a more intense impact of migraine on the emotional and physical aspects of QoL is observed among women (21-25).
Overall, literature data seem to indicate that women experience a stronger impact on both consumption of healthcare resources and QoL due to migraine (21-25). However, existing evidence is limited and relevant results are often heterogeneous (13-25). All this confirms the need of a structured data collection from a large patient population, mostly at national level, in order to evaluate the socioeconomic impact of migraine as well as to detect any difference between genders.
Objectives
The objective of the present analysis is to evaluate the socioeconomic impact of migraine in Italy, with a special focus on the detection of potential differences between male and female subjects. In particular, direct medical and non-medical costs borne by the patients (i.e. the so-called Out-of-Pocket – OoP – costs), as well as social costs due to loss of productivity and informal care will be estimated. Finally, the impact of migraine on QoL will also be assessed.
Methods
Study design
The study was conducted using a cross-sectional design. The web survey was administered by a company (Pepe Research, https://www.peperesearch.it) which selected respondents from its own database according to the following inclusion criteria:
– age ≥ 18 years old;
– confirmed diagnosis of migraine;
– episodic migraine (EM) with at least four attacks monthly or CM.
Data were collected via a web-based platform (pre-arranged in June 2018) which included a socioeconomic questionnaire and two questionnaires on QoL, namely the EuroQol 5D 5L (EQ-5D 5L) (26) and Migraine-Specific Questionnaire (MSQ v.2.1) (27). The survey was pre-tested online on a sample of 27 respondents, who had the chance to report possible comprehension problems and difficulties in the questionnaire completion. This phase did not identify any issues or difficulties in executing the tasks.
Socioeconomic questionnaire
The socioeconomic questionnaire was organized in five sections, for a total of 25 questions: (i) clinical history (questions 1-6); (ii) occupational status (questions 7-9); (iii) informal assistance (questions 10-16); (iv) visits, exams and treatments (questions 17-22); (v) loss of productivity (questions 23-25).
All questions in the survey were close-ended, as the answer is selecting one of several options or expressing a numerical quantity (e.g. number of visits) or a specific amount (e.g. cost of caregiver).
Costs incurred by the patients
Based on the data collected through the questionnaire it has been possible to estimate the quarterly OoP costs sustained by migraine patients in the last 3 months, including visits, exams, drugs which are not reimbursed by the Italian National Health Service (iNHS) and non-medical treatments. The cost incurred by patients at each visit or exam also included the cost for transport and the cost for out-of-home meal calculated on the basis of the answers to the questionnaire.
Loss of productivity (human capital approach)
From a societal perspective, it is important to take into account the loss of working productivity due to pain or discomfort or caused by the need for patients to undergo visits, exams or even hospitalizations. Such losses were evaluated on the basis of the average yearly salary, according to the human capital approach (28). Each lost working hour, estimated on a quarterly basis, was evaluated on the average hourly income for the relevant professional category (29). Values were updated to 2018. The national collective agreement for employing housemaids was used as a reference for housewives (30). The average hourly income was €31.2 for a manager, €20.6 for an entrepreneur/freelancer, €14.4 for an office worker, €12.4 for other self-employed professionals, €10.50 for labourers and €6.50 for housewives. Time lost by retirement was not considered in the analysis, as this would not have been consistent with the human capital approach (28). The total productivity loss per single patient was calculated by multiplying the average hourly wage by the number of lost working hours in the last 3 months. Based on the data released by the Ministry of Health, an average headache duration of 5.1 days with a loss of 8 working hours daily was assumed in case of hospitalization (31).
Informal assistance (replacement value approach)
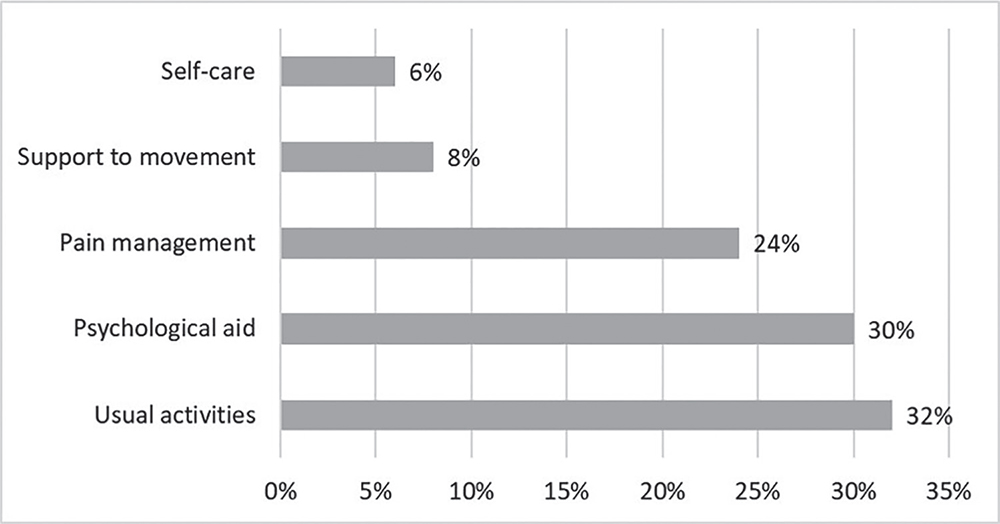
The questionnaire also investigated the need of ‘informal’ assistance, namely the unpaid assistance delivered by relatives or friends of a sick person who take care of him/her, providing help in performing daily activities and in the management of the disease (exams, medical visits, therapies, etc.) and also offering important emotional support. In case the participants stated that they need help from an informal assistant in their daily life, the calculation of the loss of productivity suffered by the caregivers was done using the replacement value approach according to the specific activities they perform and the gross yearly income for the relating profession. This approach values informal care using the same economic values (e.g. salaries, wages) attributable to those professionals who, in the market, provide similar activities (e.g. nurse) (32). In particular, the collective agreement of annual salary of nurses (€33,064) (33), carers (€12,565) (30), housemaids (€11,870) (34) and psychologists (€58,212) (33) was respectively considered for nursing-like activities, support to movement and personal care, support to usual activities and psychological aid. For each day of informal assistance received by patients, 8 hours of support were counted. The total informal assistance cost per patient was calculated by multiplying the number of hours of received assistance by the relative weight of the activity (from 0% to 100%) and its hourly cost based on the reference salary for the specific activity.
QoL questionnaires
The EQ-5D 5L is a standardized questionnaire enabling to measure the health status of the interviewed individuals and their QoL (26). The EQ-5D 5L is based on a simple and short questionnaire aimed to investigate the health status as perceived by the patient with respect to five dimensions: (i) mobility; (ii) self-care; (iii) usual activities; (iv) pain or discomfort; (v) anxiety or depression. The answer to each dimension is given on one of five levels. Eventually, the calculation of the final score (utility coefficient u) is enabled by an algorithm, based on the weight attributed to each answer. A higher score corresponds to a better health status, with 0 representing the worst health status and 1 representing the best.
The MSQ – Migraine-Specific Quality of Life Questionnaire (v.2.1) is a 14-item questionnaire that assesses QoL across three dimensions: (i) interruption of daily activities due to migraine (Role Restrictive – RR); (ii) limitation of them (Role Preventive – RP); (iii) impact on the emotional sphere of the individual (Emotional Function – EF) (27). The possible answers are: none of the time (1 point), a little bit of the time (2 points), some of the time (3 points), a good bit of the time (4 points), most of the time (5 points), all of the time (6 points). The sum of the scores of the first seven items corresponds to the raw score of the RR dimension, the sum of the scores of items 8 to 11 corresponds to the raw score of the RP dimension, while the sum of the scores of the last three items corresponds to the raw score of the EF dimension. The raw scores of the three dimensions are then rescaled from a 0 to 100 scale, such that higher scores indicate better QoL.
While the EQ-5D 5L is a non-specific questionnaire, which means it can be used regardless of the investigated disease, the MSQ is specifically designed to assess the QoL of patients with migraine.
Statistical analysis
The data reported throughout the text and in the tables are presented as average values or percentage values. The significance gender’s difference was assessed using Mann-Whitney test for non-normal distributions and chi-square test for proportions. A multivariate regression was also performed in order to investigate the impact of some factors on OoP costs, productivity losses and cost for informal care. Values with p < 0.05 were considered statistically significant.
Results
Socioeconomic questionnaire
Sample description
Six hundred and seven participants took part in the survey, with an average age of 42 years (range: 18-77) and a higher proportion of women (n = 426; 70%) than men (n = 181; 30%). Forty-seven per cent of the sample is located in Northern Italy, 36% in the South and islands, and the remaining 16% in Central Italy. Fifty-four per cent of the interviewed had obtained a high middle school diploma, 32% had an undergraduate or graduate degree, 8% had obtained a lower middle school diploma and 6% had a masters or PhD degree.
The main characteristics of migraine episodes are reported in Table I. Although the average monthly number of migraine episodes is not significantly different between women and men (7.0 vs. 7.6, respectively; p = 0.850), the duration of the attack (4-72 hours) is significantly much longer in women than in men (71% vs. 49%; p < 0.001). Yet no between-gender difference is found with regard to symptoms most frequently preceding or accompanying the attack such as photophobia (32%), phonophobia (23%) and scintillating scotoma (19%). The most frequent manifestations associated with migraine are throbbing pain (70%), discomfort to light and/or noise exposure (69%), moderate or severe pain (60%) and unilateral pain (58%). Women were more likely than men to report moderate or severe pain (63% vs. 52%; p = 0.012), worsening of symptoms due to physical activity (41% vs. 27%; p = 0.001), nausea and/or vomit (56% vs. 29%; p < 0.001) and discomfort to light and/or noise exposure (73% vs. 57%; p < 0.001). Forty-two per cent of the total sample reported that they suffer from migraine with aura.
Thirty per cent of the sample has no professional occupation (i.e. retired, student, housewife), whereas 70% claimed an occupational status. Of these, 83% are employed (labourer, office worker, manager) and 17% are self-employed (entrepreneur, freelance, other self-employed). In most of the cases (72%), the occupation is full-time. Fifty-one per cent of respondents stated an annual income of at least €20,000. Finally, significant gender differences were found across the groups considered (<€15,000; €15,000 to €19,000; €20,000 to €29,000; ≥€30,000), with a lower income for women (p < 0.001).
Informal assistance
When they suffer from migraine, 60% of respondents stated that they receive informal assistance from a caregiving relative (spouse, cohabitant, partner, parent or son), whereas 40% of them do not receive any help. The average amount of informal assistance delivered by the caregiving relative is 4 days in a month. Men receive more assisted days than women (5.2 vs. 3.9 days, respectively; p = 0.007). Sixty-seven per cent of the caregivers are employed (either employed or self-employed), 76% of whom are full-time. The distribution of the types of assistance delivered to migraine subjects is depicted in Figure 1.
Thirteen per cent of the interviewed (with the same percentage between men and women) reported to have sought paid help in the last 3 months for housekeeping (e.g. baby sitter, housemaid, caregiver), spending an average of €452 (range: €0-€3,000). The average spending per patient, calculated across the whole survey sample, was €59 with no significant difference between men and women.
Healthcare consumption
Main healthcare services consumed per patient in the last 3 months are listed in Table II. A higher percentage of men visited a general practitioner (GP) (women: 1.1; men: 1.5; p = 0.004) or a specialist (women: 0.38; men: 0.52; p = 0.011). With the exception of cranial X-ray (women: 0.11; men: 0.17; p = 0.02) and computed tomography (CT) scan (women: 0.03; men: 0.09; p = 0.02), no gender difference is seen with regard to the average number of clinical exams performed in the last 3 months.
The time spent by most of the subjects (92%) to access a procedure ranged from 1 to 4 hours including also the total time for the transfer; 2% of respondents lost a whole day. No significant differences were detected between men and women.
| Parameter | Women
(N = 426) |
Men
(N = 181) |
Total population
(N = 607) |
p-value |
|---|---|---|---|---|
| Average monthly number of attacks (n) | 7.0 | 7.6 | 7.2 | p = 0.850 |
| Duration of migraine attack (%) | ||||
|
– few minutes |
1% (6) | 4% (7) | 2% (13) | p = 0.013 |
|
– up to 2 or 3 h |
28% (118) | 47% (85) | 33% (203) | p < 0.001 |
|
– from 4 to 24 h |
43% (184) | 40% (73) | 42% (257) | p = 0.494 |
|
– even 2 or 3 d |
28% (118) | 9% (16) | 22% (134) | p < 0.001 |
| Symptoms preceding or accompanying the attack (%) | ||||
|
– photopsia (perceived flashes of light) |
11% (45) | 11% (20) | 11% (65) | p = 1.000 |
|
– scintillating scotoma |
20% (85) | 18% (33) | 19% (118) | p = 0.569 |
|
– distorted perception of objects |
4% (19) | 5% (9) | 5% (28) | p = 0.579 |
|
– hemianopsia (loss of vision in half the visual field) |
9% (40) | 11% (20) | 10% (60) | p = 0.444 |
|
– paraesthesia (limbs falling asleep) |
10% (41) | 9% (16) | 9% (57) | p = 0.703 |
|
– speech disorders |
7% (28) | 7% (13) | 7% (41) | p = 1.000 |
|
– vomit |
15% (65) | 10% (19) | 14% (84) | p = 0.100 |
|
– phonophobia |
25% (108) | 19% (34) | 23% (142) | p = 0.110 |
|
– photophobia |
35% (147) | 28% (50) | 32% (197) | p = 0.094 |
|
– other |
3% (11) | 3% (5) | 3% (16) | p = 0.100 |
| Manifestations associated with migraine (%) | ||||
|
– unilateral pain |
59% (253) | 54% (98) | 58% (351) | p = 0.255 |
|
– throbbing pain |
69% (296) | 70% (126) | 70% (422) | p = 0.807 |
|
– pain severity, from moderate to severe |
63% (270) | 52% (95) | 60% (365) | p = 0.012 |
|
– symptoms worsening due to physical activity |
41% (175) | 27% (49) | 35% (224) | p = 0.001 |
|
– nausea and/or vomit |
56% (237) | 29% (52) | 48% (289) | p < 0.001 |
|
– discomfort to light/noise exposure |
73% (313) | 57% (103) | 69% (416) | p < 0.001 |
| Subjects with migraine with aura (%) | 44% (189) | 36% (66) | 42% (255) | p = 0.068 |
Based on the cost of the co-pay fee (the so-called ‘ticket’ for public healthcare visits/exams) or the private fee (for private visits/exams), the average expenditure for visits or exams in the last 3 months was €66 (women: €58; men: €80; p = 0.005). The average costs for transport (e.g. bus, streetcar, underground, train, taxi, parking, fuel, toll) and an out-of-home meal were €12 and €8 for a single visit or exam, respectively (all calculations included a possible accompanying person).
| Parameter | Women | Men | Total population | p-value |
|---|---|---|---|---|
| Avg. no. of visits per patient in the last 3 months | ||||
|
– general practitioner |
1.10 | 1.50 | 1.20 | p = 0.004 |
|
– specialist |
0.38 | 0.52 | 0.40 | p = 0.011 |
|
– access to emergency |
0.19 | 0.12 | 0.20 | p = 0.11 |
|
– hospitalization |
0.04 | 0.03 | 0.04 | p = 0.6 |
| Avg. no. of exams per patient in the last 3 months | ||||
|
– cranial X-ray |
0.11 | 0.17 | 0.13 | p = 0.02 |
|
– electroencephalography |
0.12 | 0.16 | 0.13 | p = 0.06 |
|
– CT scan |
0.12 | 0.18 | 0.14 | p = 0.06 |
|
– magnetic resonance |
0.13 | 0.16 | 0.14 | p = 0.22 |
|
– cardiac CT scan |
0.03 | 0.09 | 0.05 | p = 0.02 |
|
– cardiac magnetic resonance |
0.04 | 0.04 | 0.04 | p = 0.40 |
|
– lumbar puncture |
0.02 | 0.00 | 0.01 | p = 0.06 |
| Average time spent for a visit or exam | ||||
|
– approx. 1 h |
27% | 30% | 28% | p = 0.45 |
|
– approx. 2 h |
37% | 32% | 35% | p = 0.24 |
|
– 2-4 h |
28% | 32% | 29% | p = 0.32 |
|
– 4-6 h |
7% | 5% | 6% | p = 0.36 |
|
– whole day |
2% | 2% | 2% | p = 1.00 |
| Cost of visits/exams | ||||
|
– avg. cost of per exam/visit |
€58 | €80 | €66 | p = 0.005 |
|
– avg. cost of transport |
€13 | €12 | €12 | p = 0.71 |
|
– avg. cost of out-of-home meal |
€7 | €10 | €8 | p = 0.55 |
| Average cost of non-iNHS-reimbursed drugs | €45 | €61 | €50 | p = 0.001 |
| Average cost of non-medical treatments | ||||
|
– acupuncture |
€2 | €4 | €3 | p = 0.49 |
|
– yoga |
€4 | €4 | €4 | p = 0.89 |
|
– postural training |
€14 | €16 | €14 | p = 0.89 |
|
– osteopathy |
€9 | €13 | €10 | p = 0.13 |
|
– progressive muscle relaxation |
€2 | €5 | €3 | p = 0.01 |
|
– homeopathic medicine |
€9 | €11 | €10 | p = 0.95 |
|
– biofeedback |
€1 | €1 | €1 | p = 0.34 |
|
– stress management |
€3 | €4 | €3 | p = 0.58 |
|
– neck manipulation techniques |
€13 | €27 | €17 | p = 0.08 |
|
– cognitive behavioural techniques |
€2 | €0 | €2 | p = 0.81 |
CT = computed tomography, iNHS = Italian National Health Service.
Because of migraine, men spent more than women to purchase drugs that are not reimbursed by the iNHS (women: €45; men: €61; p = 0.001) and non-medical treatments (women: €59; men: €83; p = 0.001) in the last 3 months (Tab. II).
Loss of productivity
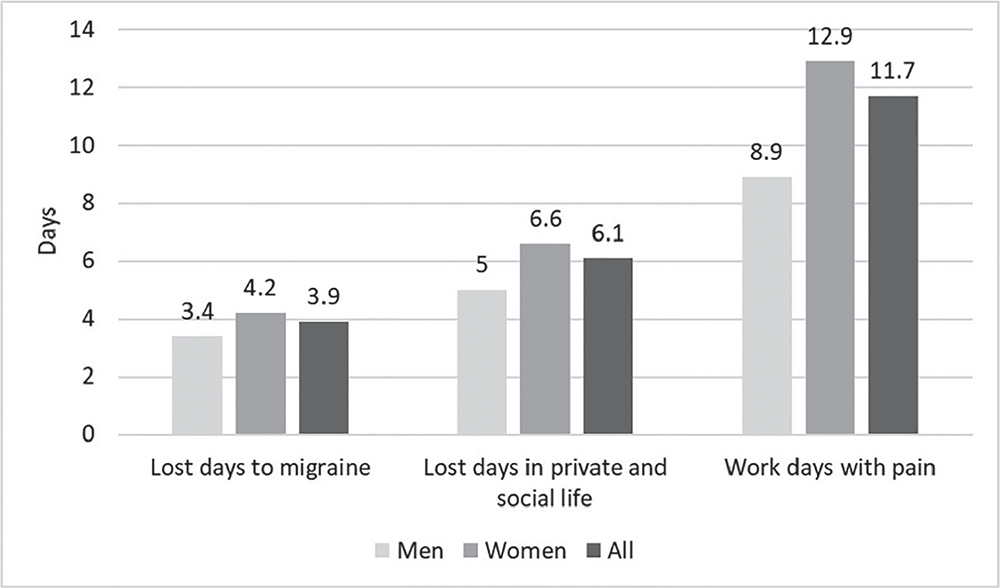
Overall, because of migraine, the subjects in the sample lost an average of 3.9 either professional or in-house work days in the last 3 months due to pain or discomfort (women: 4.2; men: 3.4; p = 0.51), 6.1 days of activity in their private and social lives (e.g. going out with friends, hobbies, sports, family activity, etc.) (women: 6.6; men: 5.0; p = 0.30), and they worked either in or out of home (including housework) for 11.7 days while they were suffering from pain or discomfort (women: 12.9; men: 8.9; p = 0.004) (Fig. 2).
Average cost for the 3-month period
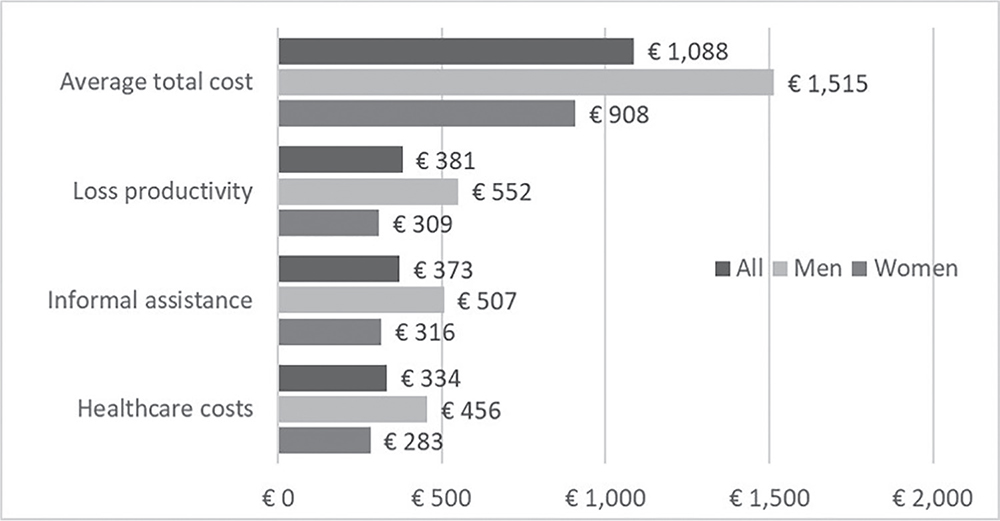
The quarterly cost resulting from the sum of the OoP costs with informal assistance and loss of productivity averaged out at €1,088 and was higher for men than it was for women (€1,515 vs. €908; p < 0.001) (Fig. 3).
These three expense categories account for approximately one-third of the total cost each: the average OoP expenditure per patient is €334 (women: €283; men: €456; p = 0.003), whereas the average expenditure for informal assistance is €373 (women: €316; men: €507; p = 0.0004) and the average loss of productivity equals €381 (women: €309; men: €552; p < 0.0001).
Quality of life
The results of the evaluation of QoL in migraine patients through the completion of the EQ-5D 5L and MSQ are summarized in Table III. The average utility coefficient calculated through the EQ-5D 5L is 0.721, with no significant between-gender difference.
In contrast, according to the results of the MSQ, a significantly worse QoL was seen in women in relation to the RR dimension (interruption of daily activities due to migraine) and the RP dimension (limitation of daily activities due to migraine) (Tab. III).
| QoL | Women | Men | Total population | p-value |
|---|---|---|---|---|
| EQ-5D | 0.717 | 0.729 | 0.721 | n.s. |
| MSQ | ||||
|
– RR |
46.8 | 53.6 | 48.8 | p < 0.001 |
|
– RP |
60.2 | 64.1 | 61.4 | p = 0.024 |
|
– EF |
59.2 | 62.9 | 60.3 | n.s. |
EF = Emotional Function; EQ-5D = EuroQol 5D; MSQ = Migraine-Specific Questionnaire; n.s. = non-significant; QoL = quality of life; RP = Role Preventive; RR = Role Restrictive.
Regression analysis
Regression analyses (Tab. IV) showed that OoP expenses and productivity losses are statistically significantly associated with gender (women incur lower expenses and report lower productivity losses), annual income (the higher the income, the greater the expenses incurred and the loss of productivity), symptoms (subjects with a higher number of attacks per month incur higher expenses) and QoL (the better the QoL, the lower the cost). Moreover, subjects with migraine with aura incur higher OoP expenses.
The cost of informal care, that is, provided in general by relatives who take care of the person suffering from migraine, was significantly associated only with the female gender, with a lower cost than the male gender.
Discussion
Limited socioeconomic evidence is available in literature regarding gender differences in patients with migraine, especially in the Italian context. Therefore, in order to at least partially fill this gap, a multidimensional survey was conducted in Italy through the administration of three questionnaires to 607 adult patients suffering from at least four migraine attacks per month. More in detail, direct medical and non-medical OoP costs, informal care and loss of productivity-related costs arising from migraine attacks and the impact of these on patients’ QoL have been evaluated, with a focus on potential gender differences.
| Parameters | Dependent variable = OoP costs* | Dependent variable = productivity loss* | Dependent variable = cost for informal assistance* | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Regression coefficient | Standard error | p-value | Regression coefficient | Standard error | p-value | Regression coefficient | Standard error | p-value | |
| Gender (Female vs. Male) | −0.184 | 0.068 | 0.007 | −0.463 | 0.214 | 0.031 | −0.860 | 0.265 | 0.001 |
| Type of migraine (with aura vs. without aura) | 0.182 | 0.063 | 0.004 | 0.339 | 0.196 | 0.084 | 0.263 | 0.243 | 0.28 |
| Gross annual income* | 0.063 | 0.019 | 0.001 | 1.029 | 0.060 | <0.001 | −0.047 | 0.074 | 0.527 |
| Number of migraine attacks per month | 0.021 | 0.007 | 0.004 | 0.066 | 0.023 | 0.004 | 0.015 | 0.028 | 0.6 |
| Utility coefficient (EuroQol-VAS) | −0.004 | 0.002 | 0.017 | −0.016 | 0.005 | 0.003 | −0.005 | 0.007 | 0.432 |
| Constant | 1.873 | 0.176 | – | 0.715 | 0.551 | – | 4.579 | 0.682 | – |
The coefficients indicate the variation of the dependent variable according to the variation of one unit for continuous parameters or towards the other class for binary parameters.
EuroQol-VAS = Euro Quality of Life Visual Analogue Scale; OoP = out of pocket.
*Logarithmic transformation
No gender difference was observed as for the monthly number of migraine episodes, approximately one every 4 days. However, significant differences are there with regard to the duration, as an attack lasting from 2 to 3 days is reported by 28% of women compared to 9% of men. No difference was detected with regard to symptoms, whereas manifestations associated with migraine (pain severity; symptoms worsening due to physical activity, nausea and/or vomit; discomfort to light and/or noise exposure) contribute to a more complex and more serious clinical presentation in women.
Around 90% of men claimed to be workers, compared to only 60% of women, who in their professions are less rewarded than men.
The survey showed that 60% of patients receive informal assistance from their relatives, for an amount of 4 days in a month on average (5.2 vs. 3.9 days for male and female patients, respectively; p = 0.007). Also, 13% of the subjects seek paid help for housekeeping.
In contrast with material previously published (13-16), men generally reported a higher utilization of healthcare resources than women with regard to visits (GP or specialist) and exams (cranial X-ray and CT).
Based on the results of a previous study conducted in Italy (12), one would have expected a higher number of days lost to migraine among men. Yet, this survey shows a higher number of lost working days and lost social activity days among women than men (4.2 and 6.6 days for women, 3.4 and 5.0 for men; p = 0.51 and 0.30, respectively), whereas at the same time women tend to go to work in a condition of illness more frequently than men (women: 12.9 days; male: 8.9 days; p = 0.004). This could be due to longer duration of the attacks and more complex clinical presentation with regard to migraine-associated manifestations in women.
The average treatment cost over the three surveyed months was shown to be higher for men than it was for women in a ratio of 1:1.5 (women: €908; men: €1,515; p < 0.001). This finding is also confirmed by another study conducted in Italy (12) in which, despite cost categories not exactly the same used in the present survey, a higher average treatment cost was found for men during the 3 months of observation (women: €2,631 €; men: €3,885), with an identical ratio of 1:1.5 (12).
The individual cost categories of healthcare costs, informal assistance and loss of productivity account for one-third of the total cost each, a proportion which remains unchanged when the results are analysed according to gender. The €173 difference between men and women in healthcare costs can be explained by a higher frequency of visits and exams among men, and the €191 difference for informal assistance is due to the higher number of assisted days required by men than by women (men: 5.2 days; women: 3.9 days; p = 0.007). Finally, although a higher number of lost working days is associated with women, the €243 incremental difference associated with men should be read in light of the lesser occupational status (60% of women vs. 90% of men) and lower average income of women (35).
The processing results of the MSQ show a significant reduction of QoL in women compared to men with regard to the evaluation of the emotional and physical domains. In contrast, probably because the domains of a non-MSQ don’t have the power to detect possible gender differences, the EQ-5D 5L results have not shown any (women: 0.717; men: 0.729; p = 0.92). However, if we compare these results to the Italian general population data (women: 0.906; men: 0.932 in the 46-55 years age group) (36), the negative impact of migraine on QoL of healthy subjects can be noticed. The comparison with other diseases is also meaningful, in that, for example, the 0.72 average utility score associated with migraine is lower than that estimated for subjects with diabetes (0.84-0.89) (37,38) or asthma (0.88) (39).
Finally, regression analyses show that OoP expenses and productivity losses are influenced by gender, income and QoL; in this context women report lower expenses and productivity losses than men due to their lower annual income. A better QoL showed a reduction of expenses and productivity losses.
The main limitation of the present analysis lies in not having considered the costs covered by the iNHS for the management of migraine patients, thus underestimating the actual average cost. Also costs covered by possible social insurance have not been included in the present analysis. Yet, it must be pointed out that the objective of this survey was to evaluate the economic impact of migraine both on society and the patients themselves. Another limitation relates to the selection of the respondents. As they were recruited via an online survey, this population may be biased towards the ability to use a computer or a mobile device with internet access (40).
Furthermore, compared to previous studies conducted nationwide (12,41), a higher number of patients were included in the present survey and they were recruited according to homogeneity for territories. The potential to gather accurate numerical data and to study a wide population of subjects is important and beneficial for quantitative data collection (42).
Conclusions
The results of the survey confirm the heavy burden of migraine on society and the patients themselves, in terms of both economic impact and QoL.
These results seem to prove, indeed, that migraine is a gender disease. A potentially unequal access to informal assistance and healthcare resources not covered by the iNHS is highlighted for women because of their lower average income and purchasing power compared to men. Women lose more days of work and social life, go to work with pain or discomfort more often, present worse manifestations of migraine and QoL. Men, on the other hand, experience higher levels of utilization and expenditure for visits and exams and, by virtue of their higher wage levels, suffer higher costs due to loss of productivity.
Disclosures
Financial support: This research was made possible by an unconditional grant from Novartis Farma.
Conflict of interest: All authors declare that there are no conflicts of interest. MN and DC are full-time employees of Novartis Farma.
References
- 1. Dodick DW. Migraine. Lancet. 2018;391(10127):1315-1330. Medline
- 2. Marconi E, Pecchioli S, Nica M, et al. Epidemiology and determinants of chronic migraine: a real-world cohort study, with nested case-control analysis, in primary care in Italy. Cephalalgia. 2020;40(5):461-469. Medline
- 3. I.H.S. Classification criteria for migraine. [Cited March 2020]; Online
- 4. Lipton RB, Serrano D, Pavlovic JM, et al. Improving the classification of migraine subtypes: an empirical approach based on factor mixture models in the American Migraine Prevalence and Prevention (AMPP) Study. Headache. 2014;54(5):830-849. Medline
- 5. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211-1259. Medline
- 6. Steiner TJ, Stovner LJ, Vos T, Jensen R, Katsarava Z. Migraine is first cause of disability in under 50s: will health politicians now take notice? J Headache Pain. 2018;19(1):17. Medline
- 7. Roncolato M, Fabbri L, Recchia G, et al. An epidemiological study to assess migraine prevalence in a sample of Italian population presenting to their GPs. Eur Neurol. 2000;43(2):102-106. Medline
- 8. Stovner Lj, Hagen K, Jensen R, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007;27(3):193-210. Medline
- 9. Berg J. Economic evidence in migraine and other headaches: a review. Eur J Health Econ. 2004;5(1)(suppl 1):S43-S54. Medline
- 10. Andlin-Sobocki P, Jönsson B, Wittchen HU, Olesen J. Cost of disorders of the brain in Europe. Eur J Neurol. 2005;12(1)(suppl 1):1-27. Medline
- 11. Vetvik KG, MacGregor EA. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017;16(1):76-87. Medline
- 12. D’Amico D, Grazzi L, Curone M, Leonardi M, Raggi A. Cost of medication overuse headache in Italian patients at the time-point of withdrawal: a retrospective study based on real data. Neurol Sci. 2017;38(suppl 1):3-6. Medline
- 13. Bezov,D, Buse DC, Stewart WF, et al. Gender differences in headache-related disability and resource utilization in episodic and episodic probable migraine: results from the American migraine prevalence and prevention study (AMPP) Headache 2010. Abstract Conference: 52nd Annual Scientific Meeting of the American-Headache-Society, Volume: 50 Online
- 14. Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies. Headache. 2015;55(1):21-34. Medline
- 15. Rhee TG, Harris IM. Gender differences in the use of complementary and alternative medicine and their association with moderate mental distress in U.S. adults with migraines/severe headaches. Headache. 2017;57(1):97-108. Medline
- 16. Wu J, Noxon V, Lu ZK. Patterns of use and health expenses associated with triptans among adults with migraines. Clin J Pain. 2015;31(8):673-679. CrossRef Medline
- 17. Manack A, Buse DC, Serrano D, et al. Lost productive time and cost due to headache in chronic (CM) and episodic migraine (EM): results: from the AMPP study. J Headache Pain. 2010;11(suppl 1):S1-S64. Online
- 18. Rastenytė D, Mickevičienė D, Stovner LJ, Thomas H, Andrée C, Steiner TJ. Prevalence and burden of headache disorders in Lithuania and their public-health and policy implications: a population-based study within the Eurolight Project. J Headache Pain. 2017;18(1):53. CrossRef Medline
- 19. Serrano D, Manack AN, Reed ML, Buse DC, Varon SF, Lipton RB. Cost and predictors of lost productive time in chronic migraine and episodic migraine: results from the American Migraine Prevalence and Prevention (AMPP) Study. Value Health. 2013;16(1):31-38. CrossRef Medline
- 20. Steiner TJ, Stovner LJ, Katsarava Z, et al. The impact of headache in Europe: principal results of the Eurolight project. J Headache Pain. 2014;15(1):31. CrossRef Medline
- 21. Baladón L, Rubio-Valera M, Serrano-Blanco A, Palao DJ, Fernández A. Gender differences in the impact of mental disorders and chronic physical conditions on health-related quality of life among non-demented primary care elderly patients. Qual Life Res. 2016;25(6):1461-1474. CrossRef Medline
- 22. Rencz F, Brodszky V, Péntek M, Bereczki D, Gulácsi L. Health state utilities for migraine based on attack frequency: a time trade-off study. Neurol Sci. 2015;36(2):197-202. CrossRef Medline
- 23. Sharma K, Remanan R, Singh S. Quality of life and psychiatric co-morbidity in Indian migraine patients: a headache clinic sample. Neurol India. 2013;61(4):355-359. CrossRef Medline
- 24. Talarska D, Zgorzalewicz-Stachowiak M. The influence of selected factors on the quality of life of children with headaches. Adv Med Sci. 2007;52(suppl 1):123-125. Medline
- 25. Zimmer T, Møller C, Westergaard M, et al. EHMTI-0209. Headache management is more than just managing pain. J Headache Pain. 2014;15:C28. CrossRef
- 26. EQ-5D-5L. Online: Online [Cited March 2020].
- 27. Migraine-specific Quality-of-life questionnaire (MSQ Version 2.1) Online: Online [Cited March 2020].
- 28. Tarricone R. Cost-of-illness analysis. What room in health economics? Health Policy. 2006;77(1):51-63. CrossRef Medline
- 29. Report Banca d’Italia. Online: Online [Cited March 2020].
- 30. Contratto Collettivo del Lavoro Domestico. Online: Online [Cited March 2020].
- 31. Degenza media per cefalea adulti, dati SDO Ministero 2016 Online: Online
- 32. van den Berg B, Brouwer WB, Koopmanschap MA. Economic valuation of informal care. An overview of methods and applications. Eur J Health Econ. 2004;5(1):36-45. CrossRef Medline
- 33. Conto Annuale del Tesoro. Ministero dell’Economia e delle Finanze. Online: Online [Cited March 2020].
- 34. Stipendi minimi. Online: Online [Cited March 2020].
- 35. La vita delle donne e degli uomini in Europa. Un ritratto statistico. Online: Online [Cited March 2020].
- 36. Scalone L, Cortesi PA, Ciampichini R, et al. Health Related Quality of Life norm data of the general population in Italy: results using the EQ-5D-3L and EQ-5D-5L instruments. Epidemiol Biostat Public Health. 2015;12(3):e11457. CrossRef
- 37. Wong ELY, Xu RH, Cheung AWL. Measurement of health-related quality of life in patients with diabetes mellitus using EQ-5D-5L in Hong Kong, China. Qual Life Res. 2020;29(7):1913-1921 CrossRef Medline
- 38. Abedini MR, Bijari B, Miri Z, Shakhs Emampour F, Abbasi A. The quality of life of the patients with diabetes type 2 using EQ-5D-5 L in Birjand. Health Qual Life Outcomes. 2020;18(1):18. CrossRef Medline
- 39. Hernandez G, Garin O, Dima AL, et al; ASTRO-LAB Group. EuroQol (EQ-5D-5L) validity in assessing the quality of life in adults with asthma: cross-sectional study. J Med Internet Res. 2019;21(1):e10178. CrossRef Medline
- 40. Bethlehem J. Selection bias in web surveys. Int Stat Rev. 2010;78(2):161-188. CrossRef
- 41. Berra E, Sances G, De Icco R, et al. Cost of chronic and episodic migraine. A pilot study from a tertiary headache centre in northern Italy. J Headache Pain. 2015;16(1):532. CrossRef Medline
- 42. Johnson EB, Onwuegbuzie AJ. Mixed methods research: a research paradigm whose time has come. Educ Res. 2004;33(7):14-26. CrossRef